Carle Cancer Center and University of Illinois College of Medicine, Urbana, Illinois.
Radiation Therapy Oncology Group Statistical Center, Philadelphia, Pennsylvania.
Int J Radiat Oncol Biol Phys. 2014 Apr 1;88(5):1092-9. doi: 10.1016/j.ijrobp.2013.12.050.
To investigate pulmonary function test (PFT) results and arterial blood gas changes (complete PFT) following stereotactic body radiation therapy (SBRT) and to see whether baseline PFT correlates with lung toxicity and overall survival in medically inoperable patients receiving SBRT for early stage, peripheral, non-small cell lung cancer (NSCLC).
During the 2-year follow-up, PFT data were collected for patients with T1-T2N0M0 peripheral NSCLC who received effectively 18 Gy × 3 in a phase 2 North American multicenter study (Radiation Therapy Oncology Group [RTOG] protocol 0236). Pulmonary toxicity was graded by using the RTOG SBRT pulmonary toxicity scale. Paired Wilcoxon signed rank test, logistic regression model, and Kaplan-Meier method were used for statistical analysis.
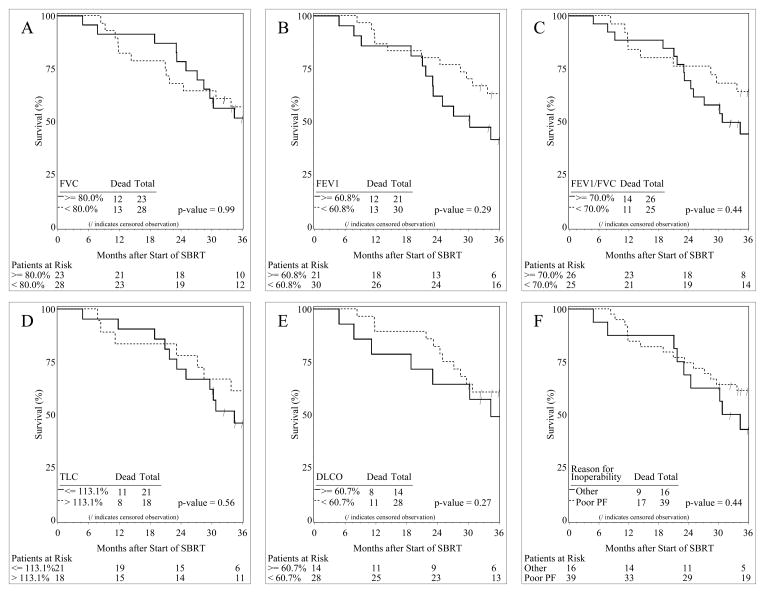
At 2 years, mean percentage predicted forced expiratory volume in the first second and diffusing capacity for carbon monoxide declines were 5.8% and 6.3%, respectively, with minimal changes in arterial blood gases and no significant decline in oxygen saturation. Baseline PFT was not predictive of any pulmonary toxicity following SBRT. Whole-lung V5 (the percentage of normal lung tissue receiving 5 Gy), V10, V20, and mean dose to the whole lung were almost identical between patients who developed pneumonitis and patients who were pneumonitis-free. Poor baseline PFT did not predict decreased overall survival. Patients with poor baseline PFT as the reason for medical inoperability had higher median and overall survival rates than patients with normal baseline PFT values but with cardiac morbidity.
Poor baseline PFT did not appear to predict pulmonary toxicity or decreased overall survival after SBRT in this medically inoperable population. Poor baseline PFT alone should not be used to exclude patients with early stage lung cancer from treatment with SBRT.
研究立体定向体部放射治疗(SBRT)后肺功能检查(PFT)结果和动脉血气变化(完整 PFT),并观察无法手术的早期周围型非小细胞肺癌(NSCLC)患者接受 SBRT 治疗时,基线 PFT 是否与肺毒性和总生存率相关。
在 2 年的随访期间,对在北美多中心 2 期研究(放射治疗肿瘤学组 [RTOG] 方案 0236)中接受有效 18 Gy×3 治疗的 T1-T2N0M0 周围型 NSCLC 患者收集 PFT 数据。采用 RTOG SBRT 肺毒性分级标准对肺毒性进行分级。采用配对 Wilcoxon 符号秩检验、逻辑回归模型和 Kaplan-Meier 法进行统计学分析。
2 年时,平均预计用力呼气量第一秒百分比和一氧化碳弥散量下降分别为 5.8%和 6.3%,动脉血气变化最小,氧饱和度无明显下降。基线 PFT 不能预测 SBRT 后任何肺毒性。发生肺炎和无肺炎患者的全肺 V5(接受 5 Gy 的正常肺组织百分比)、V10、V20 和全肺平均剂量几乎相同。基线 PFT 较差不能预测总生存率降低。因基线 PFT 较差而无法手术的患者的中位和总生存率均高于基线 PFT 值正常但存在心脏疾病的患者。
在无法手术的人群中,基线 PFT 较差似乎不会预测 SBRT 后的肺毒性或总生存率降低。单独的基线 PFT 较差不应用于排除 SBRT 治疗早期肺癌患者。