Hughes M, Moore T, Manning J, Wilkinson J, Dinsdale G, Roberts C, Murray A, Herrick A L
Centre for Musculoskeletal Research, The University of Manchester, Salford Royal NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom.
Centre for Musculoskeletal Research, The University of Manchester, Salford Royal NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom; Department of Rheumatology, Salford Royal NHS Foundation Trust, Salford, United Kingdom.
Microvasc Res. 2017 May;111:32-36. doi: 10.1016/j.mvr.2016.12.008. Epub 2016 Dec 24.
In patients with systemic sclerosis (SSc), fingertip digital ulcers (DUs) are believed to be ischaemic, and extensor surface DUs a result of mechanical factors/microtrauma. Our aim was to assess blood flow response to topical glyceryl trinitrate (GTN) compared to placebo in SSc DUs, looking for differences in pathophysiology between fingertip and extensor lesions.
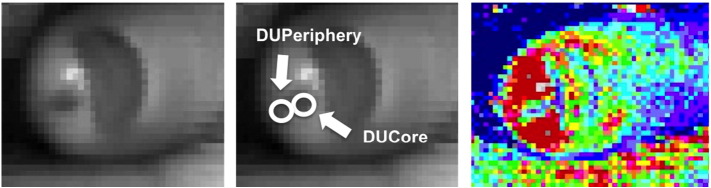
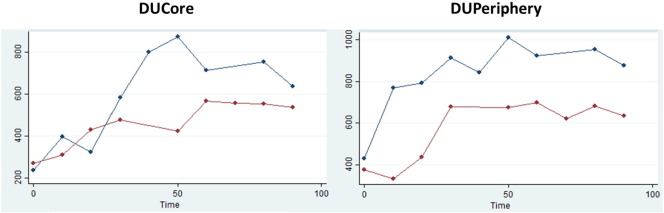
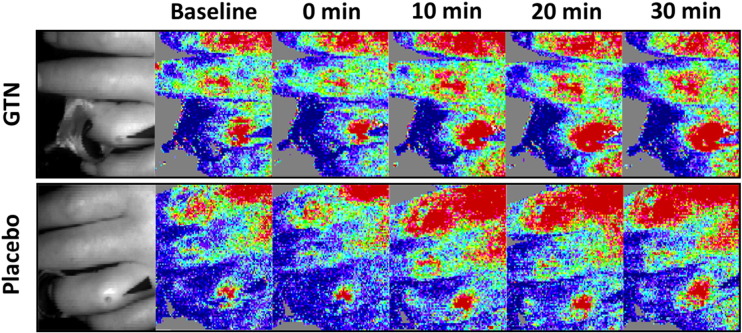
This was a double-blind, randomised, crossover, placebo-controlled study. Sixteen (6 fingertip, 10 extensor) DUs were each studied twice (one day apart): once with GTN and once with placebo ointment. Perfusion at the DU centre ('DUCore') and periphery ('DUPeriphery'), as measured by laser Doppler imaging was performed before and immediately after ointment application, then every 10min, up to 90min post-application. We calculated the area under the response curve (AUC) and the ratio of peak perfusion to baseline, then compared these between GTN and placebo.
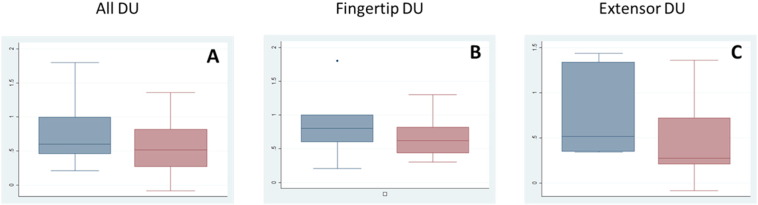
Perfusion was lower in the DUCore compared to the DUPeriphery (ratio of 0.52). The microvessels of the DUCore were responsive to GTN, with an increase in perfusion, with a similar effect in both fingertip and extensor DUs. The AUC and peak/baseline perfusion difference in means (ratio, 95% confidence interval) between GTN and placebo at the DUCore were 1.2 (1.0-1.6) and 1.2 (1.0-1.5) respectively, and at the DUPeriphery were 1.1 (0.8-1.6) and 1.0 (0.9-1.2) respectively.
DUs (both fingertip and extensor) were responsive to topical GTN, with an increase in perfusion to the ischaemic DU centre. If both fingertip and extensor DUs have a (potentially reversible) ischaemic aetiology, this has important treatment implications.
在系统性硬化症(SSc)患者中,指尖指端溃疡(DUs)被认为是缺血性的,而伸肌表面的DUs是机械因素/微创伤所致。我们的目的是评估与安慰剂相比,局部应用硝酸甘油(GTN)对SSc患者DUs的血流反应,以寻找指尖和伸肌损伤在病理生理学上的差异。
这是一项双盲、随机、交叉、安慰剂对照研究。16个指端溃疡(6个指尖溃疡,10个伸肌表面溃疡)每个均进行两次研究(间隔一天):一次使用GTN,一次使用安慰剂软膏。在涂抹软膏前和涂抹后立即,然后每10分钟直至涂抹后90分钟,通过激光多普勒成像测量溃疡中心(“DUCore”)和周边(“DUPeriphery”)的灌注。我们计算了反应曲线下面积(AUC)以及峰值灌注与基线的比值,然后比较GTN和安慰剂之间的这些指标。
与DUPeriphery相比,DUCore的灌注较低(比值为0.52)。DUCore的微血管对GTN有反应,灌注增加,指尖和伸肌DUs的效果相似。GTN和安慰剂在DUCore处的AUC以及平均峰值/基线灌注差异(比值,95%置信区间)分别为1.2(1.0 - 1.6)和1.2(1.0 - 1.5),在DUPeriphery处分别为1.1(0.8 - 1.6)和1.0(0.9 - 1.2)。
指端溃疡(包括指尖和伸肌表面)对局部应用GTN有反应,缺血性的溃疡中心灌注增加。如果指尖和伸肌DUs都有(潜在可逆的)缺血病因,这具有重要的治疗意义。