Cui Qiuxia, Li Zhihua, Kong Deguang, Wang Kun, Wu Gaosong
Department of Thyroid and Breast Surgery, Tongji Hospital, Huazhong University of Science and Technology, Wuhan, P.R. China.
Medicine (Baltimore). 2016 Dec;95(52):e5810. doi: 10.1097/MD.0000000000005810.
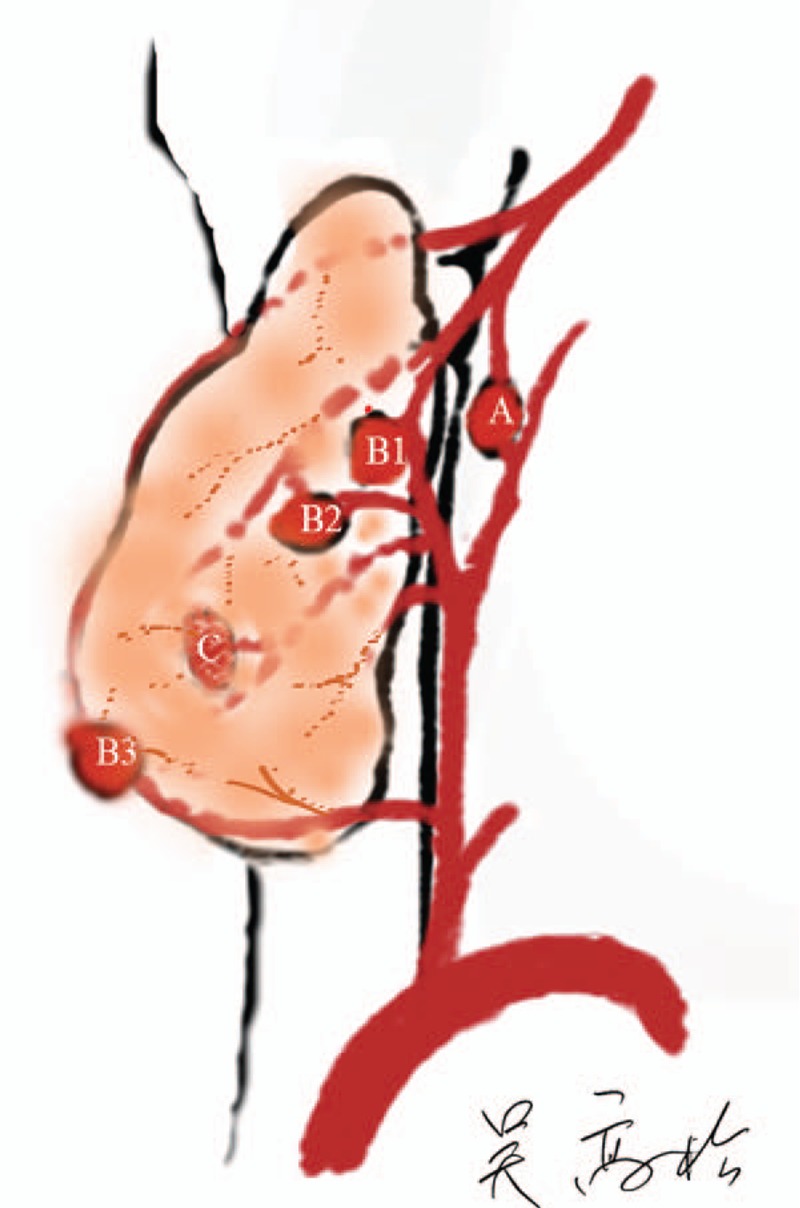
The best method of preventing hypoparathyroidism after thyroidectomy is to keep parathyroid glands in situ. However, hypoparathyroidism still regularly occurs with the existing parathyroid classification system, and the incidence of permanent hypoparathyroidism has not been reduced. We created a novel system for classifying parathyroid glands that can guide parathyroid preservation in thyroidectomy.We prospectively observed parathyroid glands using the new system in 218 neck surgeries, compared with 132 under the traditional system from January 2014 to September 2015 at a single clinic center. Briefly, we classified parathyroid glands as follows: Type A, no dependency on the thyroid; B1, partial blood supply from the thyroid but retains adequate blood supply after removal of the thyroid; B2, partial blood supply from the thyroid and becomes devascularized after the removal of the thyroid; B3, blood supply mostly from the thyroid; and C, blood supply completely dependent on the thyroid. The classifications were used to decide between in situ preservation or auto-transplantation.The most common type of parathyroid gland was type B1 (53.77%), followed by type A (20.89%), which are the perfect categories for in situ preservation. Type B2 (17.52%) and type B3 (1.21%) have a chance to be kept in situ. For type C (6.61%), in situ preservation is impossible. When in-situ preservation is ruled out, parathyroid auto-transplantation is an alternative, with partial or total gland tissue, depending on the classification and the surgeon's discretion. Among the patients who were classified under the new system, 43.6% presented with transient hypoparathyroidism (symptoms lasting ≤6 months) after surgery, versus 42.4% in the old system, which was not a significant difference. However, permanent hypothyroidism (symptoms lasting >6 months) was not detected in the applied group, but in 3.0% of patients in the nonapplied group (P = 0.01).Our novel functional nomenclature system for parathyroid glands can provide a guide for preserving parathyroid function. For certain types, such as type B2 and C, instead of being kept in situ, auto-transplantation of partial or total parathyroid tissue is a prudent choice to ensure continued function.
甲状腺切除术后预防甲状旁腺功能减退的最佳方法是保留甲状旁腺原位。然而,在现有的甲状旁腺分类系统下,甲状旁腺功能减退仍经常发生,永久性甲状旁腺功能减退的发生率并未降低。我们创建了一种新的甲状旁腺分类系统,可在甲状腺切除术中指导甲状旁腺的保留。2014年1月至2015年9月,我们在单一临床中心前瞻性地使用新系统观察了218例颈部手术中的甲状旁腺,并与传统系统下的132例进行了比较。简而言之,我们将甲状旁腺分类如下:A型,不依赖甲状腺;B1型,部分血液供应来自甲状腺,但甲状腺切除后仍保留充足血液供应;B2型,部分血液供应来自甲状腺,甲状腺切除后血供中断;B3型,血液供应主要来自甲状腺;C型,血液供应完全依赖甲状腺。这些分类用于决定原位保留还是自体移植。最常见的甲状旁腺类型是B1型(53.77%),其次是A型(20.89%),这两种类型是原位保留的理想类别。B2型(17.52%)和B3型(1.21%)有机会原位保留。对于C型(6.61%),不可能原位保留。当排除原位保留时,甲状旁腺自体移植是一种选择,根据分类和外科医生的判断,可移植部分或全部腺体组织。在新系统分类的患者中,43.6%术后出现短暂性甲状旁腺功能减退(症状持续≤6个月),旧系统组为42.4%,差异无统计学意义。然而,应用组未检测到永久性甲状腺功能减退(症状持续>6个月),而非应用组有3.0%的患者出现(P = 0.01)。我们新的甲状旁腺功能命名系统可为保留甲状旁腺功能提供指导。对于某些类型,如B2型和C型,与其原位保留,甲状旁腺部分或全部组织的自体移植是确保其持续功能的明智选择。