Department of Medicine, Stanford University, Stanford, California2Departments of Health Research and Policy, Stanford University, Stanford, California.
Department of Systems, Populations, and Leadership and Institute for Healthcare Policy and Innovation, University of Michigan School of Nursing, Ann Arbor.
JAMA Oncol. 2017 Mar 1;3(3):391-397. doi: 10.1001/jamaoncol.2016.5652.
Advances in the evaluation and treatment of breast cancer have made the clinical decision-making context much more complex. A second opinion from a medical oncologist may facilitate decision making for women with breast cancer, yet little is known about second opinion use.
To investigate the patterns and correlates of second opinion use and the effect on chemotherapy decisions.
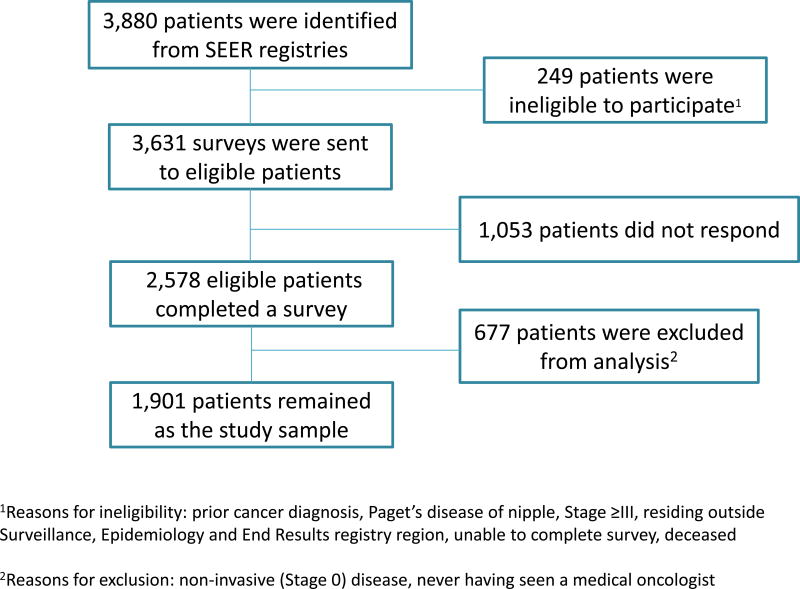
DESIGN, SETTING, AND PARTICIPANTS: A total of 1901 women newly diagnosed with stages 0 to II breast cancer between July 2013 and September 2014 (response rate, 71.0%) were accrued through 2 population-based Surveillance, Epidemiology, and End Results registries (Georgia and Los Angeles County, California) and surveyed about their experiences with medical oncologists, decision making, and chemotherapy use.
Factors associated with second opinion use were evaluated using logistic regression. Also assessed was the association between second opinion and chemotherapy use, adjusting for chemotherapy indication and propensity for receiving a second opinion. Multiple imputation and weighting were used to account for missing data.
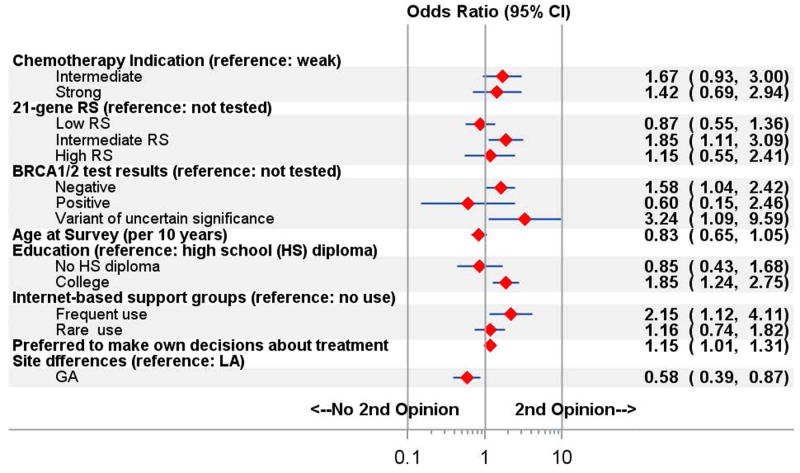
A total of 1901 patients with stage I to II breast cancer (mean [SD] age, 61.6 [11.0] years; 1071 [56.3%] non-Hispanic white) saw any medical oncologist. Analysis of multiply imputed, weighted data (mean n = 1866) showed that 168 (9.8%) (SE, 0.74%) received a second opinion and 54 (3.2%) (SE, 0.47%) received chemotherapy from the second oncologist. Satisfaction with chemotherapy decisions was high and did not differ between those who did (mean [SD], 4.3 [0.08] on a 1- to 5-point scale) or did not (4.4 [0.03]) obtain a second opinion (P = .29). Predictors of second opinion use included college education vs less education (odds ratio [OR], 1.85; 95% CI, 1.24-2.75), frequent use of internet-based support groups (OR, 2.15; 95% CI, 1.12-4.11), an intermediate result on the 21-gene recurrence score assay (OR, 1.85; 95% CI, 1.11-3.09), and a variant of uncertain significance on hereditary cancer genetic testing (OR, 3.24; 95% CI, 1.09-9.59). After controlling for patient and tumor characteristics, second opinion use was not associated with chemotherapy receipt (OR, 1.04; 95% CI, 0.71-1.52).
Second opinion use was low (<10%) among patients with early-stage breast cancer, and high decision satisfaction regardless of second opinion use suggests little unmet demand. Along with educational level and use of internet support groups, uncertain results on genomic testing predicted second opinion use. Patient demand for second opinions may increase as more complex genomic tests are disseminated.
乳腺癌评估和治疗方面的进展使得临床决策环境变得更加复杂。来自医学肿瘤学家的第二意见可能有助于乳腺癌患者的决策,但对第二意见的使用知之甚少。
调查第二意见使用的模式和相关性,以及对化疗决策的影响。
设计、地点和参与者:共有 1901 名新诊断为 0 期至 2 期乳腺癌的女性(应答率为 71.0%)通过 2 个基于人群的监测、流行病学和最终结果登记处(佐治亚州和加利福尼亚州洛杉矶县)入组,并对她们与医学肿瘤学家的接触、决策和化疗使用情况进行了调查。
使用逻辑回归评估与第二意见使用相关的因素。还评估了第二意见与化疗使用之间的关联,调整了化疗指征和接受第二意见的倾向。使用多重插补和加权来解释缺失数据。
共有 1901 名 I 期至 II 期乳腺癌患者(平均[标准差]年龄为 61.6[11.0]岁;1071[56.3%]为非西班牙裔白人)见过任何医学肿瘤学家。对多重插补、加权数据(平均 n=1866)的分析显示,168 名(9.8%)(SE,0.74%)患者获得了第二意见,54 名(3.2%)(SE,0.47%)患者从第二肿瘤学家处接受了化疗。化疗决策的满意度很高,并且获得(平均[标准差],4.3[0.08],1 到 5 分制)或未获得(4.4[0.03])第二意见的患者之间没有差异(P=0.29)。第二意见使用的预测因素包括大学教育与较低的教育水平(比值比[OR],1.85;95%置信区间[CI],1.24-2.75)、经常使用基于互联网的支持小组(OR,2.15;95% CI,1.12-4.11)、21 基因复发评分检测的中等结果(OR,1.85;95% CI,1.11-3.09)和遗传性癌症基因检测的不确定意义变异(OR,3.24;95% CI,1.09-9.59)。在控制患者和肿瘤特征后,第二意见的使用与化疗的接受无关(OR,1.04;95% CI,0.71-1.52)。
早期乳腺癌患者中第二意见的使用比例较低(<10%),并且无论是否使用第二意见,满意度都很高,这表明需求未得到满足。除了教育水平和互联网支持小组的使用外,基因组检测不确定的结果也预示着第二意见的使用。随着更多复杂的基因组检测的传播,患者对第二意见的需求可能会增加。