Niikura Ryota, Nagata Naoyoshi, Doyama Hisashi, Ota Ryosuke, Ishii Naoki, Mabe Katsuhiro, Nishida Tsutomu, Hikichi Takuto, Sumiyama Kazuki, Nishikawa Jun, Uraoka Toshio, Kiyotoki Shu, Fujishiro Mitsuhiro, Koike Kazuhiko
Ryota Niikura, Mitsuhiro Fujishiro, Kazuhiko Koike, Department of Gastroenterology, Graduate School of Medicine, the University of Tokyo, Bunkyo-ku, Tokyo 113-8655, Japan.
World J Gastrointest Endosc. 2016 Dec 16;8(20):785-794. doi: 10.4253/wjge.v8.i20.785.
To clarify the current state of practice for colonic diverticular bleeding (CDB) in Japan.
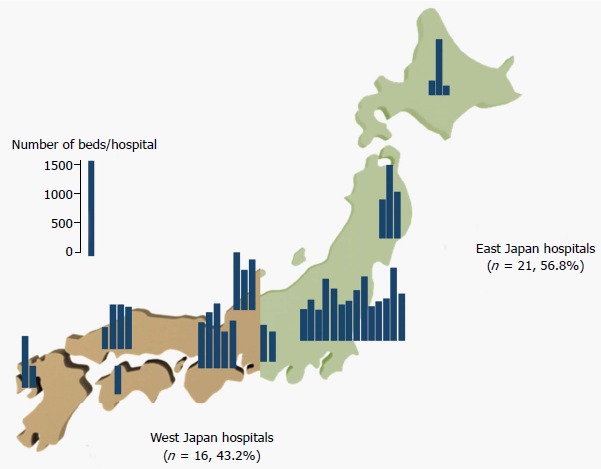
We conducted multicenter questionnaire surveys of the practice for CDB including clinical settings (8 questions), diagnoses (8 questions), treatments (7 questions), and outcomes (4 questions) in 37 hospitals across Japan. The answers were compared between hospitals with high and low number of inpatient beds to investigate which factor influenced the answers.
Endoscopists at all 37 hospitals answered the questions, and the mean number of endoscopists at these hospitals was 12.7. Of all the hospitals, computed tomography was performed before colonoscopy in 67% of the hospitals. The rate of bowel preparation was 46.0%. Early colonoscopy was performed within 24 h in 43.2% of the hospitals. Of the hospitals, 83.8% performed clipping as first-line endoscopic therapy. More than half of the hospitals experienced less than 20% rebleeding events after endoscopic hemostasis. No significant difference was observed in the annual number of patients hospitalized for CDB between high- (≥ 700 beds) and low-volume hospitals. More emergency visits ( = 0.012) and endoscopists ( = 0.015), and less frequent participation of nursing staff in early colonoscopy ( = 0.045) were observed in the high-volume hospitals.
Some practices unique to Japan were found, such as performing computed tomography before colonoscopy, no bowel preparation, and clipping as first-line therapy. Although, the number of staff differed, the practices for CDB were common irrespective of hospital size.
阐明日本结肠憩室出血(CDB)的当前临床实践状况。
我们对日本37家医院的CDB临床实践进行了多中心问卷调查,内容包括临床环境(8个问题)、诊断(8个问题)、治疗(7个问题)和结果(4个问题)。比较了住院床位数多和少的医院的答案,以调查哪些因素影响答案。
所有37家医院的内镜医师都回答了问题,这些医院内镜医师的平均人数为12.7人。在所有医院中,67%的医院在结肠镜检查前进行了计算机断层扫描。肠道准备率为46.0%。43.2%的医院在24小时内进行了早期结肠镜检查。在这些医院中,83.8%的医院将钳夹术作为一线内镜治疗方法。超过一半的医院在内镜止血后再出血事件发生率低于20%。高容量医院(≥700张床位)和低容量医院因CDB住院的患者年数量无显著差异。高容量医院的急诊就诊次数更多(P = 0.012)、内镜医师更多(P = 0.015),而护士参与早期结肠镜检查的频率更低(P = 0.045)。
发现了一些日本特有的做法,如在结肠镜检查前进行计算机断层扫描、不进行肠道准备以及将钳夹术作为一线治疗方法。尽管人员数量不同,但无论医院规模大小,CDB的临床实践都是常见的。