Wu Xiaomai, Zhu Yefei, Chen Qiuying, Gong Liuyang, Lin Jian, Lv Dongqing, Feng Jiaxi
Department of Respiratory Medicine, Taizhou Hospital of Zhejiang Province, Linhai 317000, China.
Operation Department, Taizhou Hospital of Zhejiang Province, Linhai 317000, China.
Biomed Res Int. 2016;2016:8395268. doi: 10.1155/2016/8395268. Epub 2016 Dec 4.
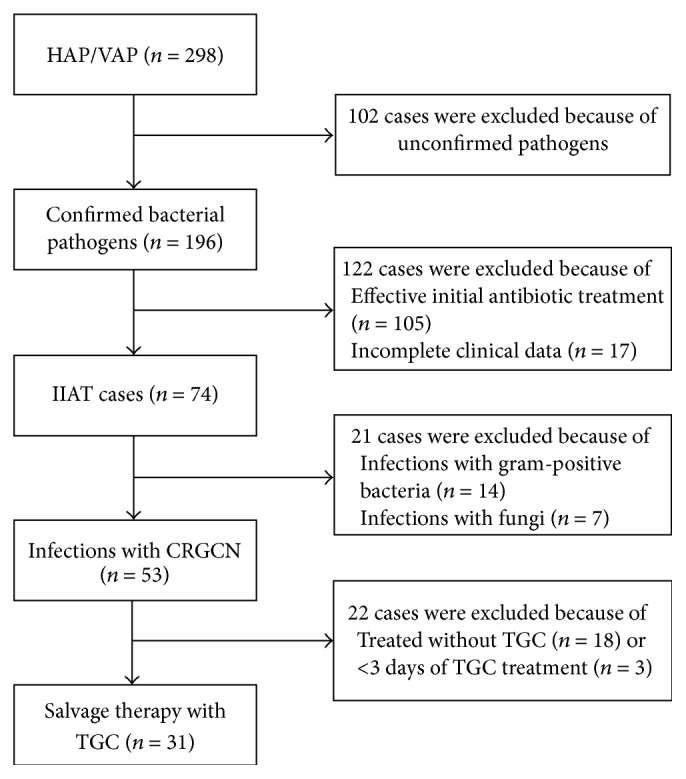
. Nosocomial pneumonia due to carbapenem-resistant Gram-negative bacteria (CRGNB) is a growing concern because treatment options are limited and the mortality rate is high. The effect of tigecycline (TGC) on nosocomial pneumonia due to CRGNB in patients who have received inappropriate initial empiric antibiotic treatment (IIAT) is unclear. Therefore, this study aimed to examine the effect of TGC on nosocomial pneumonia due to CRGNB in critically ill patients who had received IIAT. . A retrospective study was conducted in an adult respiratory intensive care unit. Data were obtained and analyzed for all patients who were treated with TGC ≥ 3 days for microbiologically confirmed nosocomial pneumonia due to CRGNB and had experienced initial antibiotic failure. Clinical and microbiological outcomes were investigated. . Thirty-one patients with hospital-acquired pneumonia or ventilator-associated pneumonia were included in the study. The majority of the responsible organisms were carbapenem-resistant (67.7%), followed by (16.1%) and (9.7%). Twenty patients were treated with high-dose TGC therapy (100 mg every 12 h after a 200 mg loading dose), and the others received a standard-dose therapy (50 mg every 12 h after a 100 mg loading dose). The duration of TGC therapy was 14.3 ± 2.8 days. The global clinical cure rate and the microbiological eradication rate were 48.4% and 61.3%, respectively. The overall ICU mortality rate was 45.2%. A higher score on the Acute Physiology and Chronic Health Evaluation II and a longer duration of IIAT were associated with clinical failure. High-dose TGC therapy had a higher clinical success rate [65.0% (13/20) versus 18.2% (2/11), = 0.023] and a lower ICU mortality rate [30.0% (6/20) versus 72.7% (8/11), = 0.031] than the standard-dose therapy. . TGC, especially a high-dose regimen, might be a justifiable option for critically ill patients with nosocomial pneumonia due to CRGNB who have received IIAT when the options for these patients are limited.
耐碳青霉烯类革兰氏阴性菌(CRGNB)引起的医院获得性肺炎日益受到关注,因为治疗选择有限且死亡率高。替加环素(TGC)对接受过不恰当初始经验性抗生素治疗(IIAT)的患者因CRGNB所致医院获得性肺炎的影响尚不清楚。因此,本研究旨在探讨TGC对接受过IIAT的重症患者因CRGNB所致医院获得性肺炎的影响。
在一家成人呼吸重症监护病房进行了一项回顾性研究。收集并分析了所有因CRGNB导致的微生物学确诊的医院获得性肺炎且初始抗生素治疗失败、接受TGC治疗≥3天的患者的数据。调查了临床和微生物学结果。
3例医院获得性肺炎或呼吸机相关性肺炎患者纳入研究。大多数病原菌对碳青霉烯类耐药(67.7%),其次是[具体病原菌1](16.1%)和[具体病原菌2](9.7%)。20例患者接受高剂量TGC治疗(负荷剂量200mg后每12小时100mg),其余患者接受标准剂量治疗(负荷剂量100mg后每12小时50mg)。TGC治疗持续时间为14.3±2.8天。总体临床治愈率和微生物清除率分别为48.4%和61.3%。ICU总体死亡率为45.2%。急性生理与慢性健康状况评价II(APACHE II)评分较高和IIAT持续时间较长与临床治疗失败相关。高剂量TGC治疗比标准剂量治疗具有更高的临床成功率[65.0%(13/20)对18.2%(2/11),P=0.023]和更低的ICU死亡率[30.0%(6/20)对72.7%(8/11),P=0.031]。
对于接受过IIAT且因CRGNB导致医院获得性肺炎的重症患者,当这些患者的治疗选择有限时,TGC尤其是高剂量方案可能是一个合理的选择。