Song Huan, Fang Fang, Valdimarsdóttir Unnur, Lu Donghao, Andersson Therese M-L, Hultman Christina, Ye Weimin, Lundell Lars, Johansson Jan, Nilsson Magnus, Lindblad Mats
Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Box 281, Stockholm, SE171 77, Sweden.
Center of Public Health Sciences, Faculty of Medicine, University of Iceland, Reykjavík, Iceland.
BMC Cancer. 2017 Jan 3;17(1):2. doi: 10.1186/s12885-016-3013-7.
Except for overall survival, whether or not waiting time for treatment could influences other domains of cancer patients' overall well-being is to a large extent unknown. Therefore, we performed this study to determine the effect of waiting time for cancer treatment on the mental health of patients with esophageal or gastric cancer.
Based on the Swedish National Quality Register for Esophageal and Gastric Cancers (NREV), we followed 7,080 patients diagnosed 2006-2012 from the time of treatment decision. Waiting time for treatment was defined as the interval between diagnosis and treatment decision, and was classified into quartiles. Mental disorders were identified by either clinical diagnosis through hospital visit or prescription of psychiatric medications. For patients without any mental disorder before treatment, the association between waiting time and subsequent onset of mental disorders was assessed by hazard ratios (HRs) with 95% confidence interval (CI), derived from multivariable-adjusted Cox model. For patients with a preexisting mental disorder, we compared the rate of psychiatric care by different waiting times, allowing for repeated events.
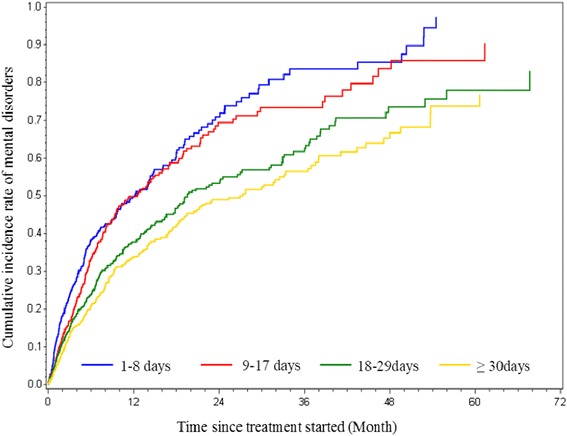
Among 4,120 patients without any preexisting mental disorder, lower risk of new onset mental disorders was noted for patients with longer waiting times, i.e. 18-29 days (HR 0.86; 95% CI 0.74-1.00) and 30-60 days (HR 0.79; 95% CI 0.67-0.93) as compared with 9-17 days. Among 2,312 patients with preexisting mental disorders, longer waiting time was associated with more frequent psychiatric hospital care during the first year after treatment (37.5% higher rate per quartile increase in waiting time; p for trend = 0.0002). However, no such association was observed beyond one year nor for the prescription of psychiatric medications.
These data suggest that waiting time to treatment for esophageal or gastric cancer may have different mental health consequences for patients depending on their past psychiatric vulnerabilities. Our study sheds further light on the complexity of waiting time management, and calls for a comprehensive strategy that takes into account different domains of patient well-being in addition to the overall survival.
除总生存期外,治疗等待时间是否会影响癌症患者总体幸福感的其他方面在很大程度上尚不清楚。因此,我们开展了这项研究,以确定癌症治疗等待时间对食管癌或胃癌患者心理健康的影响。
基于瑞典国家食管癌和胃癌质量登记处(NREV),我们对2006年至2012年确诊的7080例患者从治疗决策时开始进行随访。治疗等待时间定义为诊断与治疗决策之间的间隔,并分为四分位数。通过医院就诊的临床诊断或精神科药物处方来确定精神障碍。对于治疗前无任何精神障碍的患者,通过多变量调整的Cox模型得出的风险比(HR)及其95%置信区间(CI)来评估等待时间与随后精神障碍发病之间的关联。对于已有精神障碍的患者,我们比较了不同等待时间的精神科护理率,允许重复事件发生。
在4120例治疗前无任何精神障碍的患者中,等待时间较长的患者新发精神障碍风险较低,即与等待9 - 17天的患者相比,等待18 - 29天(HR 0.86;95% CI 0.74 - 1.00)和30 - 60天(HR 0.79;95% CI 0.67 - 0.93)的患者风险较低。在2312例已有精神障碍的患者中,等待时间较长与治疗后第一年更频繁的精神科住院护理相关(等待时间每增加一个四分位数,发生率高37.5%;趋势p = 0.0002)。然而,在一年后未观察到这种关联,精神科药物处方方面也未观察到这种关联。
这些数据表明,食管癌或胃癌的治疗等待时间可能因患者过去的精神脆弱性而对其心理健康产生不同影响。我们的研究进一步揭示了等待时间管理的复杂性,并呼吁采取一种综合策略,除了总生存期外,还要考虑患者幸福感的不同方面。