Mao Jiang-Feng, Liu Zhao-Xiang, Nie Min, Wang Xi, Xu Hong-Li, Huang Bing-Kun, Zheng Jun-Jie, Min Le, Kaiser Ursula Brigitte, Wu Xue-Yan
Department of Endocrinology, Peking Union Medical College Hospital, Key Laboratory of Endocrinology, Ministry of Health, Beijing 100730, China.
Internal Department, Division of Endocrinology, Diabetes, and Hypertension, Brigham and Women's Hospital, Harvard Medical School, Boston, MA 02115, USA.
Asian J Androl. 2017 Nov-Dec;19(6):680-685. doi: 10.4103/1008-682X.193568.
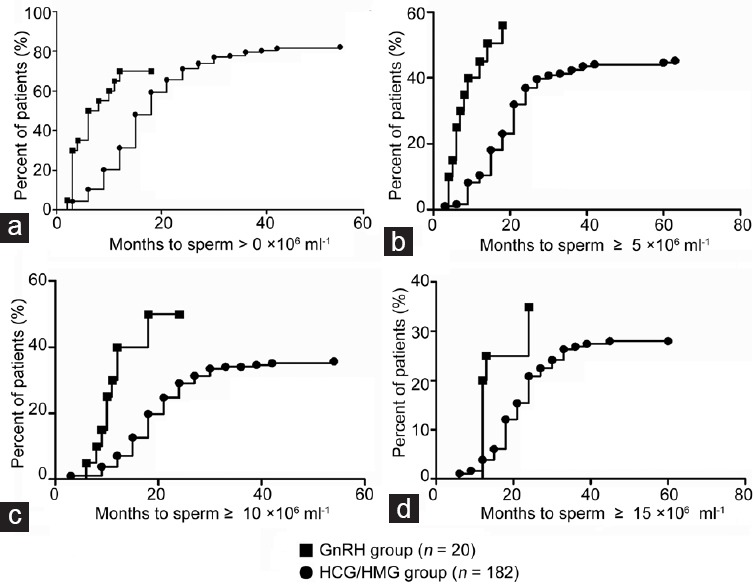
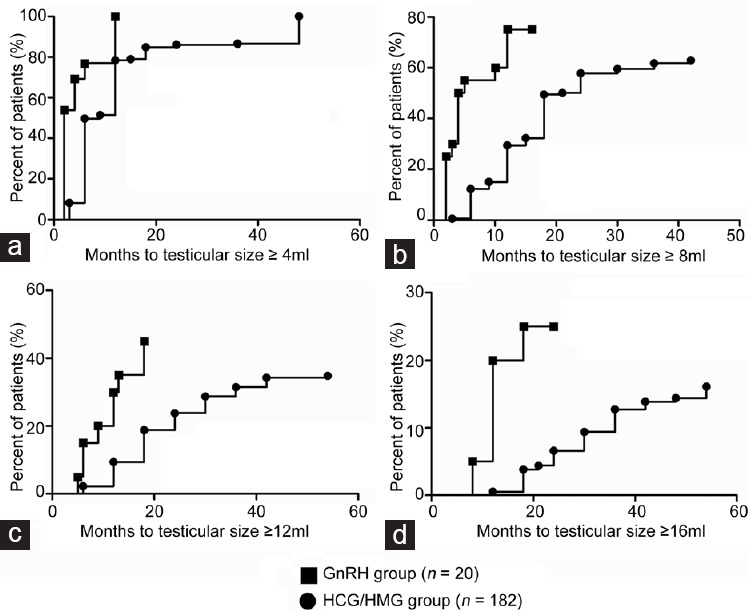
Both pulsatile gonadotropin-releasing hormone (GnRH) infusion and combined gonadotropin therapy (human chorionic gonadotropin and human menopausal gonadotropin [HCG/HMG]) are effective to induce spermatogenesis in male patients with congenital hypogonadotropic hypogonadism (CHH). However, evidence is lacking as to which treatment strategy is better. This retrospective cohort study included 202 patients with CHH: twenty had received pulsatile GnRH and 182 had received HCG/HMG. Patients had received therapy for at least 12 months. The total follow-up time was 15.6 ± 5.0 months (range: 12-27 months) for the GnRH group and 28.7 ± 13.0 months (range: 12-66 months) for the HCG/HMG group. The median time to first sperm appearance was 6 months (95% confidence interval [CI]: 1.6-10.4) in the GnRH group versus 18 months (95% CI: 16.4-20.0) in the HCG/HMG group (P < 0.001). The median time to achieve sperm concentrations ≥5 × 10 6 ml-1 was 14 months (95% CI: 5.8-22.2) in the GnRH group versus 27 months (95% CI: 18.9-35.1) in the HCG/HMG group (P < 0.001), and the median time to concentrations ≥10 × 10 6 ml-1 was 18 months (95% CI: 10.0-26.0) in the GnRH group versus 39 months (95% CI unknown) in the HCG/HMG group. Compared to the GnRH group, the HCG/HMG group required longer treatment periods to achieve testicular sizes of ≥4 ml, ≥8 ml, ≥12 ml, and ≥16 ml. Sperm motility (a + b + c percentage) evaluated in semen samples with concentrations >1 × 10 6 ml-1 was 43.7% ± 20.4% (16 samples) in the GnRH group versus 43.2% ± 18.1% (153 samples) in the HCG/HMG group (P = 0.921). Notably, during follow-up, the GnRH group had lower serum testosterone levels than the HCG/HMG group (8.3 ± 4.6 vs 16.2 ± 8.2 nmol l-1 , P < 0.001). Our study found that pulsatile GnRH therapy was associated with earlier spermatogenesis and larger testicular size compared to combined gonadotropin therapy. Additional prospective randomized studies would be required to confirm these findings.
脉冲式促性腺激素释放激素(GnRH)输注和联合促性腺激素疗法(人绒毛膜促性腺激素和人绝经期促性腺激素[HCG/HMG])对于先天性低促性腺激素性性腺功能减退(CHH)男性患者诱导精子发生均有效。然而,尚无证据表明哪种治疗策略更佳。这项回顾性队列研究纳入了202例CHH患者:20例接受了脉冲式GnRH治疗,182例接受了HCG/HMG治疗。患者接受治疗至少12个月。GnRH组的总随访时间为15.6±5.0个月(范围:12 - 27个月),HCG/HMG组为28.7±13.0个月(范围:12 - 66个月)。GnRH组首次出现精子的中位时间为6个月(95%置信区间[CI]:1.6 - 10.4),而HCG/HMG组为18个月(95%CI:16.4 - 20.0)(P<0.001)。GnRH组达到精子浓度≥5×10⁶/ml⁻¹的中位时间为14个月(95%CI:5.8 - 22.2),HCG/HMG组为27个月(95%CI:18.9 - 35.1)(P<0.001),达到浓度≥10×10⁶/ml⁻¹的中位时间,GnRH组为18个月(95%CI:10.0 - 26.0),HCG/HMG组为39个月(95%CI未知)。与GnRH组相比,HCG/HMG组达到睾丸体积≥4ml、≥8ml、≥12ml和≥16ml需要更长的治疗时间。在精子浓度>1×10⁶/ml⁻¹的精液样本中评估的精子活力(a + b + c百分比),GnRH组为43.7%±20.4%(16个样本),HCG/HMG组为43.2%±18.1%(153个样本)(P = 0.921)。值得注意的是,在随访期间,GnRH组的血清睾酮水平低于HCG/HMG组(8.3±4.6 vs 16.2±8.2 nmol/l⁻¹,P<0.001)。我们的研究发现,与联合促性腺激素疗法相比,脉冲式GnRH疗法与更早的精子发生和更大的睾丸体积相关。需要更多前瞻性随机研究来证实这些发现。