Tseng Chih-Wei, Lin Cheng-Li, Chen Yu-Tso, Jeng Long-Bin
Division of Allergy, Immunology and Rheumatology, Taichung Veterans General Hospital, Taichung, Taiwan.
Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan.
PLoS One. 2017 Jan 5;12(1):e0169070. doi: 10.1371/journal.pone.0169070. eCollection 2017.
The aim of this study was to determine whether spinal cord injuries (SCI) is associated with increased risk of ischemic bowel syndrome (IBS) in an Asian population by analyzing data from the National Health Insurance Research Database (NHIRD) in Taiwan.
Patients aged ≥20 years in the inpatient database with newly identified SCI from 2000 to 2011 were selected as the SCI cohort. For the non-SCI cohort, patients were selected based on a 1:4 risk-set sampling. Hospitalization with a new diagnosis of IBS during the follow-up was the main outcome measure. We used the standard univariable and multivariable Cox proportional hazard regression models to determine adjusted subhazard ratios (SHR) and 95% confidence interval (CI) in the SCI and non-SCI cohorts.
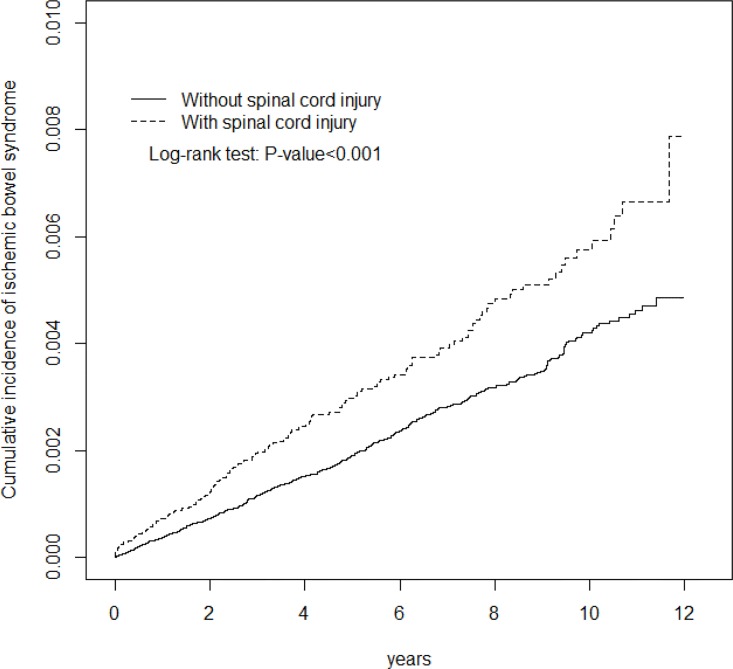
Patients with SCI were at significant risk for IBS, with an adjusted SHR (aSHR) of 1.25, 95% CI = 1.04-1.51. Multivariable analysis showed individuals with SCI were associated with a greater risk of IBS than individuals without SCI among males (aSHR = 1.47, 95% CI = 1.16-1.86), all age groups (≤49 y: aSHR = 2.15, 95% CI = 1.24-3.74; 50-65 y: aSHR = 1.82, 95% CI = 1.15-2.88; >65 y: aSHR = 1.39, 95% CI = 1.11-1.74) and those without comorbidities (aSHR = 1.41, 95% CI = 1.04-1.93). Comorbidities including diabetes, hypertension, heart failure, coronary artery disease (CAD), Stroke, and end stage renal disease (ESRD) significantly increased the risk of IBS.
Patients hospitalized for SCI have increased risks of developing IBS. Though the mechanism that predisposes SCI patients to IBS is unclear, we suggest that physicians promptly identify and treat correctable risk factors.
本研究旨在通过分析台湾地区国民健康保险研究数据库(NHIRD)的数据,确定亚洲人群中脊髓损伤(SCI)是否与缺血性肠综合征(IBS)风险增加相关。
选取2000年至2011年住院数据库中年龄≥20岁且新确诊为SCI的患者作为SCI队列。对于非SCI队列,根据1:4风险集抽样选取患者。随访期间新诊断为IBS的住院情况为主要观察指标。我们使用标准单变量和多变量Cox比例风险回归模型来确定SCI和非SCI队列中的调整后亚风险比(SHR)及95%置信区间(CI)。
SCI患者患IBS的风险显著增加,调整后SHR(aSHR)为1.25,95%CI = 1.04 - 1.51。多变量分析显示,男性中SCI患者患IBS的风险高于非SCI患者(aSHR = 1.47,95%CI = 1.16 - 1.86),各年龄组均如此(≤49岁:aSHR = 2.15,95%CI = 1.24 - 3.74;50 - 65岁:aSHR = 1.82,95%CI = 1.15 - 2.88;>65岁:aSHR = 1.39,95%CI = 1.11 - 1.74),无合并症者也如此(aSHR = 1.41,95%CI = 1.04 - 1.93)。包括糖尿病、高血压、心力衰竭、冠状动脉疾病(CAD)、中风和终末期肾病(ESRD)在内的合并症显著增加了患IBS的风险。
因SCI住院的患者患IBS的风险增加。尽管SCI患者易患IBS的机制尚不清楚,但我们建议医生及时识别并治疗可纠正的风险因素。