Xia Weiliang, Ke Qinghong, Guo Hua, Wang Weilin, Zhang Min, Shen Yan, Wu Jian, Xu Xiao, Yan Sheng, Yu Jun, Zhang Mangli, Zheng Shusen
Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, First Affiliated Hospital, School of Medicine, Zhejiang University, Qingchun Road 79, Hangzhou, 310003, China.
Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, First Affiliated Hospital, School of Medicine, Zhejiang University, Qingchun Road 79, Hangzhou, 310003, China.
BMC Cancer. 2017 Jan 5;17(1):14. doi: 10.1186/s12885-016-3028-0.
The Hangzhou criteria expand the Milan criteria safely and effectively in selecting hepatocellular carcinoma (HCC) candidates for liver transplantation (LT), but some patients exceeding the Milan but fulfilling the Hangzhou criteria still show poor outcomes due to early tumor recurrence. In this study, the platelet-to-lymphocyte ratio (PLR) was employed to differentiate high-risk tumor recurrence recipients, and a new method combining PLR and the Hangzhou criteria was established.
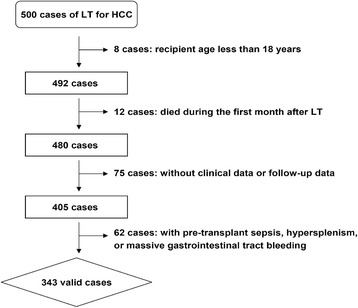
The clinical data of 343 LT for HCC were retrospectively analyzed. Receiver operating characteristic (ROC) analysis was used to determine the PLR cut-off value to stratify patients exceeding the Milan but fulfilling the Hangzhou criteria. The recurrence-free survival (RFS) of recipients was compared after stratification. The Hangzhou criteria & PLR method was proposed and its feasibility was validated by ROC analysis.
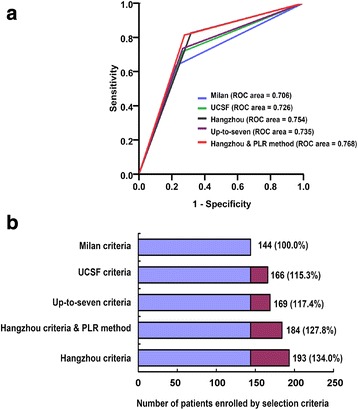
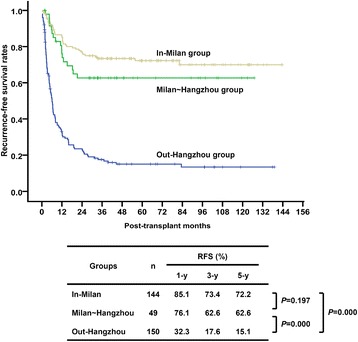
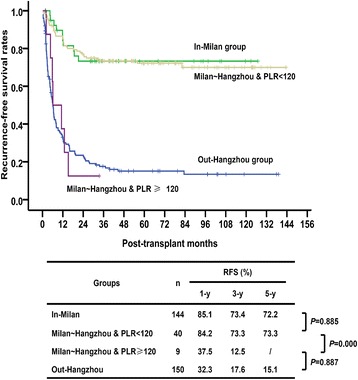
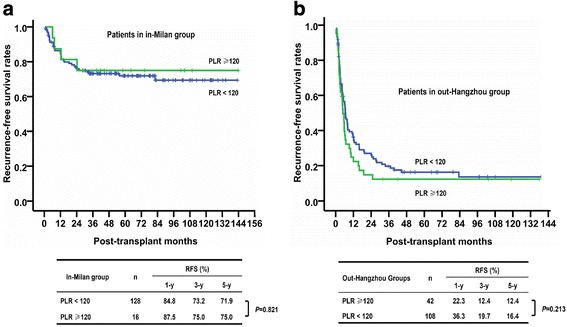
PLR 120 was the most significant cut-off value when comparing RFS of patients exceeding the Milan but fulfilling the Hangzhou criteria. After stratification, the 1-, 3-, and 5-year RFS of patients exceeding the Milan but fulfilling the Hangzhou criteria with PLR < 120 were 84.2%, 73.3%, and 73.3%, respectively, comparable with 85.7%, 73.9%, and 72.8%, respectively, in patients fulfilling the Milan criteria (P = 0.885). Patients exceeding the Milan but fulfilling the Hangzhou criteria with PLR ≥ 120 showed poor outcomes, which were similar in patients exceeding the Hangzhou criteria; 1-, 3-, and 5-year RFS were only 37.5%, 12.5%, and 12.5% vs. 32.3%, 17.6%, and 15.1%, respectively (P = 0.887). ROC analysis demonstrated that the ROC area of the Hangzhou criteria & PLR method was 0.768 for RFS. Multivariate analysis confirmed that PLR ≥ 120 was independently associated with RFS of patients exceeding the Milan but fulfilling the Hangzhou criteria.
The Hangzhou criteria combined with the pre-transplant PLR can accurately exclude high-risk tumor recurrence recipients; this approach expands the Milan criteria effectively without any sacrifice.
杭州标准在选择肝细胞癌(HCC)肝移植(LT)受者时安全有效地扩展了米兰标准,但一些超过米兰标准但符合杭州标准的患者仍因早期肿瘤复发而预后不良。在本研究中,采用血小板与淋巴细胞比值(PLR)来区分高风险肿瘤复发受者,并建立了一种将PLR与杭州标准相结合的新方法。
回顾性分析343例HCC肝移植患者的临床资料。采用受试者操作特征(ROC)分析确定PLR临界值,以对超过米兰标准但符合杭州标准的患者进行分层。比较分层后受者的无复发生存期(RFS)。提出了杭州标准&PLR方法,并通过ROC分析验证了其可行性。
在比较超过米兰标准但符合杭州标准的患者的RFS时,PLR 120是最具显著性的临界值。分层后,PLR<120的超过米兰标准但符合杭州标准的患者1年、3年和5年RFS分别为84.2%、73.3%和73.3%,与符合米兰标准的患者分别为85.7%、73.9%和72.8%相当(P = 0.885)。PLR≥120的超过米兰标准但符合杭州标准的患者预后较差,与超过杭州标准的患者相似;1年、3年和5年RFS分别仅为37.5%、12.5%和12.5%,而分别为32.3%、17.6%和15.1%(P = 0.887)。ROC分析表明,杭州标准&PLR方法的RFS的ROC面积为0.768。多因素分析证实,PLR≥120与超过米兰标准但符合杭州标准的患者的RFS独立相关。
杭州标准联合移植前PLR可准确排除高风险肿瘤复发受者;这种方法有效地扩展了米兰标准,且没有任何牺牲。