Knai Kathrine, Skjaervold Nils Kristian
Department of Circulation and Medical Imaging, Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway.
Department of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway.
BMC Res Notes. 2017 Jan 3;10(1):2. doi: 10.1186/s13104-016-2333-7.
The aim of this study was to construct a non-invasive model for acute right ventricular afterload increase by hypoxic pulmonary vasoconstriction. Intact animal models are vital to improving our understanding of the pathophysiology of acute right ventricular failure. Acute right ventricular failure is caused by increased afterload of the right ventricle by chronic or acute pulmonary hypertension combined with regionally or globally reduced right ventricular contractile capacity. Previous models are hampered by their invasiveness; this is unfortunate as the pulmonary circulation is a low-pressure system that needs to be studied in closed chest animals. Hypoxic pulmonary vasoconstriction is a mechanism that causes vasoconstriction in alveolar vessels in response to alveolar hypoxia. In this study we explored the use of hypoxic pulmonary vasoconstriction as a means to increase the pressure load on the right ventricle.
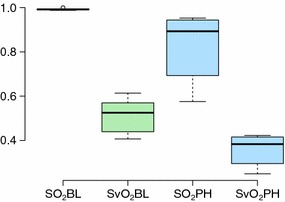
Pulmonary hypertension was induced by lowering the FiO to levels below the physiological range in eight anesthetized and mechanically ventilated pigs. The pigs were monitored with blood pressure measurements and blood gases. The mean pulmonary artery pressures (mPAP) of the animals increased from 18.3 (4.2) to 28.4 (4.6) mmHg and the pulmonary vascular resistance (PVR) from 254 (76) dyns/cm to 504 (191) dyns/cm, with a lowering of FiO from 0.30 to 0.15 (0.024). The animals' individual baseline mPAPs varied substantially as did their response to hypoxia. The reduced FiO level yielded an overall lowering in oxygen offer, but the global oxygen consumption was unaltered.
We showed in this study that the mPAP and the PVR could be raised by approximately 100% in the study animals by lowering the FiO from 0.30 to 0.15 (0.024). We therefore present a novel method for minimally invasive (closed chest) right ventricular afterload manipulations intended for future studies of acute right ventricular failure. The method should in theory be reversible, although this was not studied in this work.
本研究的目的是构建一种通过缺氧性肺血管收缩导致急性右心室后负荷增加的非侵入性模型。完整的动物模型对于增进我们对急性右心室衰竭病理生理学的理解至关重要。急性右心室衰竭是由慢性或急性肺动脉高压导致右心室后负荷增加,同时伴有局部或整体右心室收缩能力降低引起的。先前的模型因具有侵入性而受到限制;这很不幸,因为肺循环是一个低压系统,需要在闭胸动物中进行研究。缺氧性肺血管收缩是一种机制,可使肺泡血管在肺泡缺氧时发生血管收缩。在本研究中,我们探讨了利用缺氧性肺血管收缩作为增加右心室压力负荷的一种手段。
通过将八只麻醉并机械通气的猪的吸入氧分数(FiO)降至生理范围以下来诱导肺动脉高压。通过测量血压和血气对猪进行监测。动物的平均肺动脉压(mPAP)从18.3(4.2)mmHg增加到28.4(4.6)mmHg,肺血管阻力(PVR)从254(76)dyns/cm增加到504(191)dyns/cm,同时FiO从0.30降至0.15(0.024)。动物个体的基线mPAP差异很大,它们对缺氧的反应也各不相同。FiO水平降低导致总体氧供减少,但整体氧耗未改变。
我们在本研究中表明,通过将FiO从0.30降至0.15(0.024),研究动物的mPAP和PVR可升高约100%。因此,我们提出了一种用于微创(闭胸)右心室后负荷操作的新方法,旨在用于未来急性右心室衰竭的研究。理论上该方法应该是可逆的,尽管本研究未对此进行探讨。