Morise Zenichi
Zenichi Morise, Department of Surgery, Fujita Health University School of Medicine, Toyoake 470-1192, Japan.
World J Gastroenterol. 2016 Dec 21;22(47):10267-10274. doi: 10.3748/wjg.v22.i47.10267.
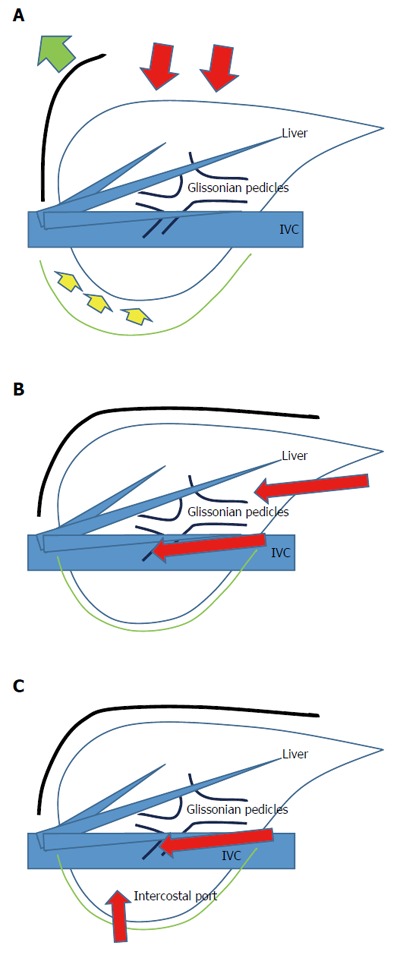
Laparoscopic liver resection (LLR) for tumors in the posterosuperior liver [segment (S) 7 and deep S6] is a challenging clinical procedure. This area is located in the bottom of the small subphrenic space (rib cage), with the large and heavy right liver on it when the patient is in the supine position. Thus, LLR of this area is technically demanding because of the handling of the right liver which is necessary to obtain a fine surgical view, secure hemostasis and conduct the resection so as to achieve an appropriate surgical margin in the cage. Handling of the right liver may be performed by the hand-assisted approach, robotic liver resection or by using spacers, such as a sterile glove pouch. In addition, the operative field of posterosuperior resection is in the deep bottom area of the subphrenic cage, with the liver S6 obstructing the laparoscopic caudal view of lesions. The use of intercostal ports facilitates the direct lateral approach into the cage and to the target area, with the combination of mobilization of the liver. Postural changes during the LLR procedure have also been reported to facilitate the LLR for this area, such as left lateral positioning for posterior sectionectomy and semi-prone positioning for tumors in the posterosuperior segments. In our hospital, LLR procedures for posterosuperior tumors are performed the caudal approach with postural changes. The left lateral position is used for posterior sectionectomy and the semi-prone position is used for S7 segmentectomy and partial resections of S7 and deep S6 without combined intercostal ports insertion. Although the movement of instruments is restricted in the caudal approach, compared to the lateral approach, port placement in the para-vertebra area makes the manipulation feasible and stable, with minimum damage to the environment around the liver.
腹腔镜肝切除术(LLR)用于治疗肝后上区(第7段和深部第6段)肿瘤是一项具有挑战性的临床手术。该区域位于小膈下间隙(肋骨笼)底部,患者仰卧时,其上有体积大且重量重的右肝。因此,该区域的LLR技术要求高,因为要获得良好的手术视野、确保止血并进行切除以在肋骨笼内获得合适的手术切缘,就必须处理右肝。处理右肝可通过手辅助方法、机器人肝切除术或使用间隔物(如无菌手套袋)来进行。此外,后上区切除术的手术视野位于膈下肋骨笼的深部底部区域,肝S6会遮挡腹腔镜对病变的尾侧视野。使用肋间端口有助于直接从侧面进入肋骨笼和目标区域,并结合肝脏游离。据报道,LLR手术过程中的体位改变也有助于该区域的LLR,如左外侧卧位用于后段切除术,半俯卧位用于后上段肿瘤切除术。在我们医院,采用尾侧入路并结合体位改变进行后上区肿瘤的LLR手术。左外侧卧位用于后段切除术,半俯卧位用于第7段切除术以及第7段和深部第6段的部分切除术,不联合插入肋间端口。尽管与侧方入路相比,尾侧入路中器械的移动受到限制,但在椎旁区域放置端口可使操作可行且稳定,对肝脏周围环境的损伤最小。