Rhodes Corinne M, Chang Yuchiao, Regan Susan, Triant Virginia A
Division of General Internal Medicine, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania, United States of America.
Division of General Internal Medicine, Massachusetts General Hospital, Boston, Massachusetts, United States of America.
PLoS One. 2017 Jan 6;12(1):e0169246. doi: 10.1371/journal.pone.0169246. eCollection 2017.
The Human Immunodeficiency Virus (HIV) epidemic has evolved, with an increasing non-communicable disease (NCD) burden emerging and need for long-term management, yet there are limited data to help delineate the optimal care model to screen for NCDs for this patient population.
The primary aim was to compare rates of NCD preventive screening in persons living with HIV/AIDS (PLWHA) by type of HIV care model, focusing on metabolic/cardiovascular disease (CVD) and cancer screening. We hypothesized that primary care models that included generalists would have higher preventive screening rates.
Prospective observational cohort study.
Partners HealthCare System (PHS) encompassing Brigham & Women's Hospital, Massachusetts General Hospital, and affiliated community health centers.
PLWHA age >18 engaged in active primary care at PHS.
HIV care model categorized as infectious disease (ID) providers only, generalist providers only, or ID plus generalist providers.
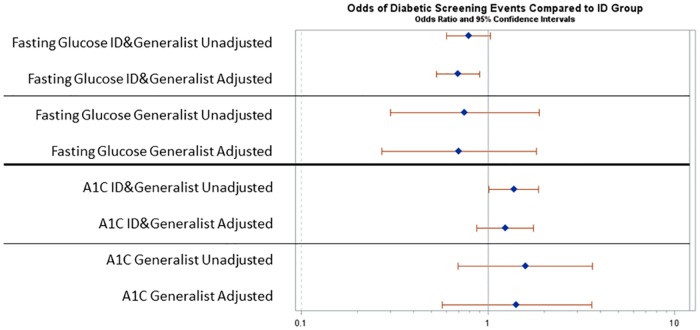
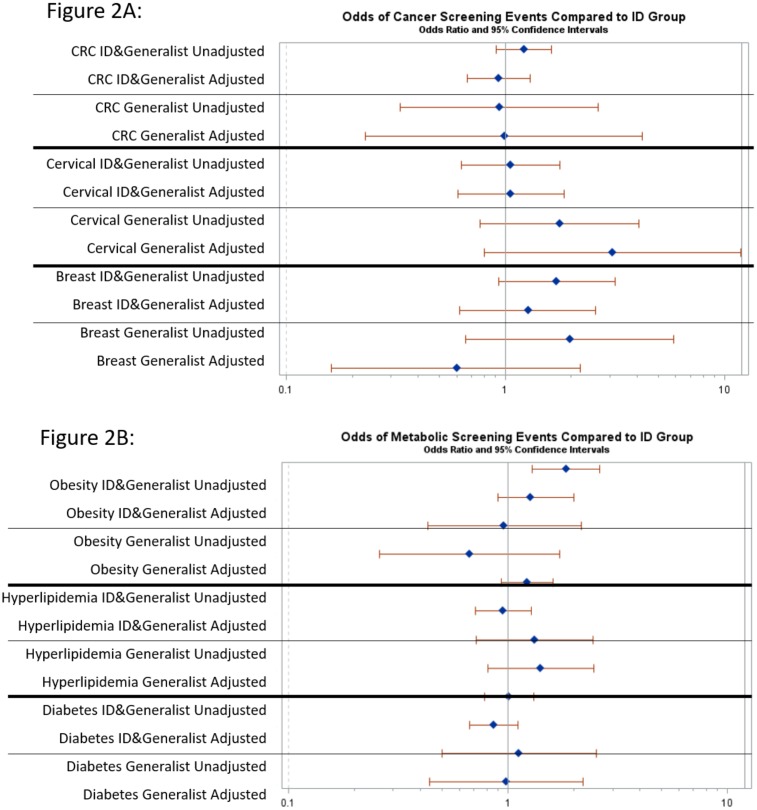
MAIN OUTCOME(S) AND MEASURES(S): Odds of screening for metabolic/CVD outcomes including hypertension (HTN), obesity, hyperlipidemia (HL), and diabetes (DM) and cancer including colorectal cancer (CRC), cervical cancer, and breast cancer.
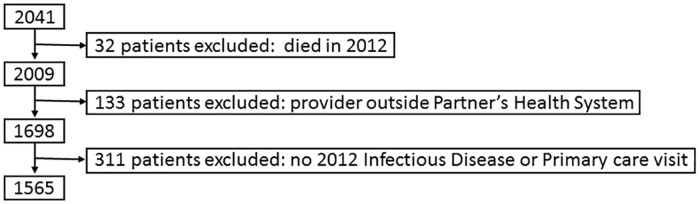
In a cohort of 1565 PLWHA, distribution by HIV care model was 875 ID (56%), 90 generalists (6%), and 600 ID plus generalists (38%). Patients in the generalist group had lower odds of viral suppression but similar CD4 counts and ART exposure as compared with ID and ID plus generalist groups. In analyses adjusting for sociodemographic and clinical covariates and clustering within provider, there were no significant differences in metabolic/CVD or cancer screening rates among the three HIV care models.
There were no notable differences in metabolic/CVD or cancer screening rates by HIV care model after adjusting for sociodemographic and clinical factors. These findings suggest that HIV patients receive similar preventive health care for NCDs independent of HIV care model.
人类免疫缺陷病毒(HIV)流行态势已发生演变,非传染性疾病(NCD)负担日益加重,且需要长期管理,但用于帮助确定针对该患者群体进行非传染性疾病筛查的最佳护理模式的数据有限。
主要目的是比较不同HIV护理模式下的HIV/AIDS患者(PLWHA)的非传染性疾病预防筛查率,重点关注代谢/心血管疾病(CVD)和癌症筛查。我们假设包含全科医生的初级护理模式会有更高的预防筛查率。
前瞻性观察性队列研究。
合作伙伴医疗保健系统(PHS),涵盖布里格姆妇女医院、马萨诸塞州总医院及附属社区健康中心。
年龄大于18岁且在PHS接受积极初级护理的PLWHA。
HIV护理模式分为仅由传染病(ID)提供者、仅由全科医生提供者或ID加全科医生提供者。
代谢/CVD结局(包括高血压(HTN)、肥胖、高脂血症(HL)和糖尿病(DM))以及癌症(包括结直肠癌(CRC)、宫颈癌和乳腺癌)的筛查几率。
在1565名PLWHA队列中,按HIV护理模式分布为875名ID提供者(56%)、90名全科医生(6%)和600名ID加全科医生提供者(38%)。与ID组和ID加全科医生组相比,全科医生组患者病毒抑制几率较低,但CD4计数和抗逆转录病毒治疗暴露情况相似。在对社会人口统计学和临床协变量以及提供者内部聚类进行调整的分析中,三种HIV护理模式在代谢/CVD或癌症筛查率方面无显著差异。
在对社会人口统计学和临床因素进行调整后,不同HIV护理模式在代谢/CVD或癌症筛查率方面无显著差异。这些发现表明,HIV患者无论HIV护理模式如何,接受的非传染性疾病预防性医疗保健相似。