Kruser Jacqueline M, Taylor Lauren J, Campbell Toby C, Zelenski Amy, Johnson Sara K, Nabozny Michael J, Steffens Nicole M, Tucholka Jennifer L, Kwekkeboom Kris L, Schwarze Margaret L
Department of Medicine and Center for Healthcare Studies, Northwestern University, Chicago, Illinois, USA.
Department of Surgery, University of Wisconsin, Madison, Wisconsin, USA.
J Pain Symptom Manage. 2017 Apr;53(4):711-719.e5. doi: 10.1016/j.jpainsymman.2016.11.014. Epub 2017 Jan 4.
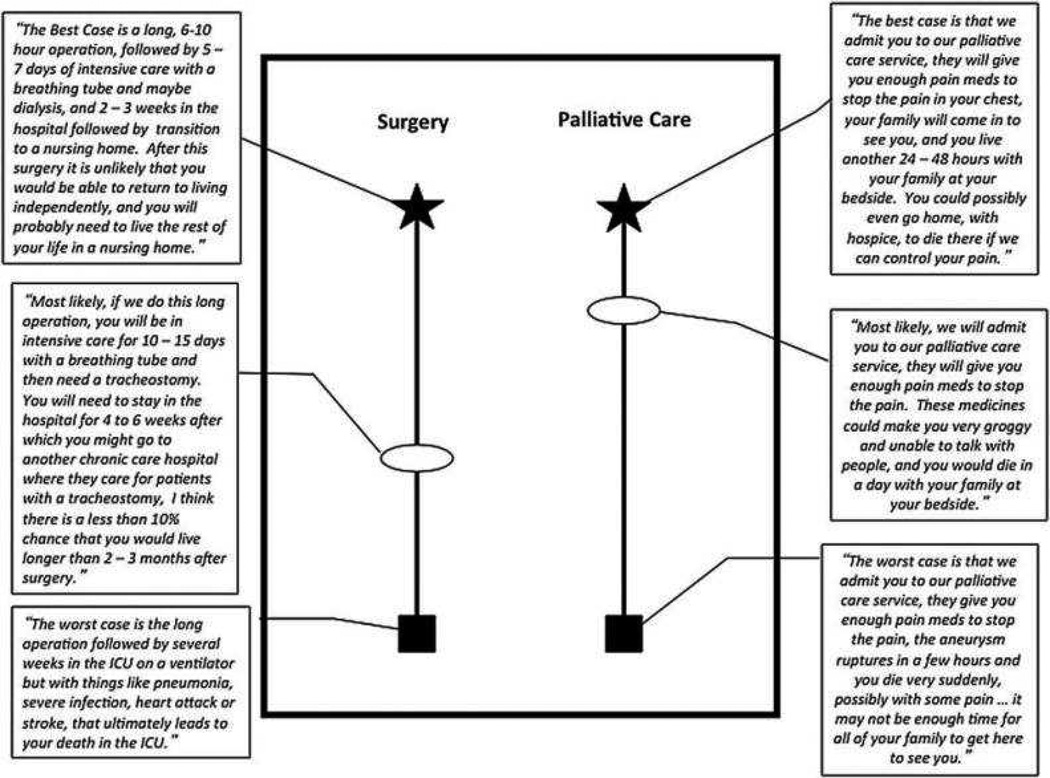
Older adults often have surgery in the months preceding death, which can initiate postoperative treatments inconsistent with end-of-life values. "Best Case/Worst Case" (BC/WC) is a communication tool designed to promote goal-concordant care during discussions about high-risk surgery.
The objective of this study was to evaluate a structured training program designed to teach surgeons how to use BC/WC.
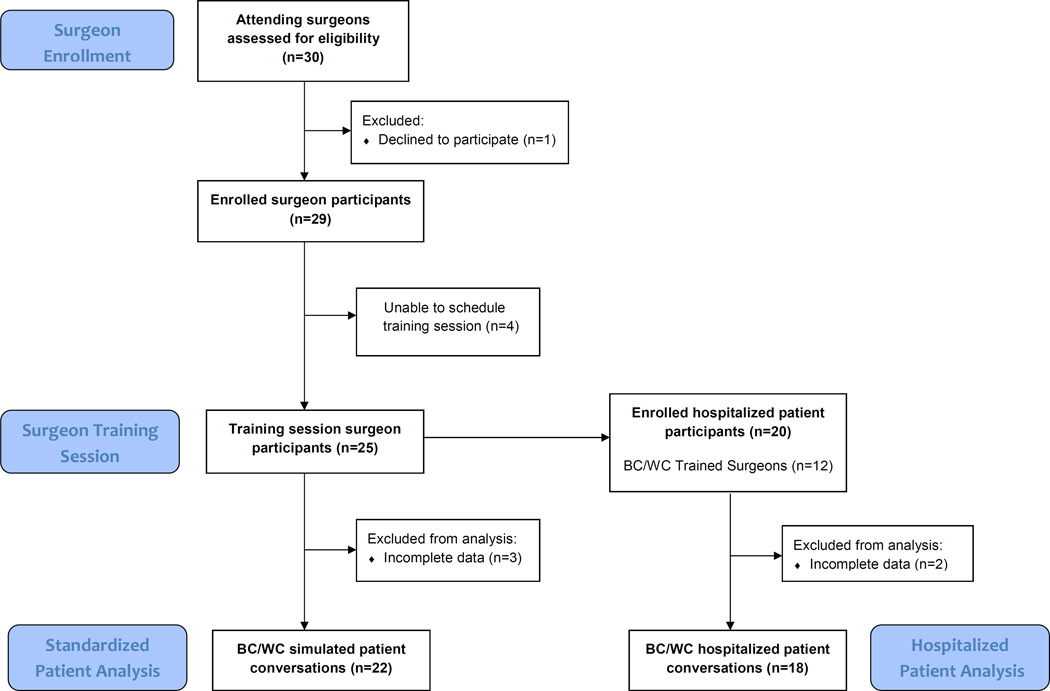
Twenty-five surgeons from one tertiary care hospital completed a two-hour training session followed by individual coaching. We audio-recorded surgeons using BC/WC with standardized patients and 20 hospitalized patients. Hospitalized patients and their families participated in an open-ended interview 30 to 120 days after enrollment. We used a checklist of 11 BC/WC elements to measure tool fidelity and surgeons completed the Practitioner Opinion Survey to measure acceptability of the tool. We used qualitative analysis to evaluate variability in tool content and to characterize patient and family perceptions of the tool.
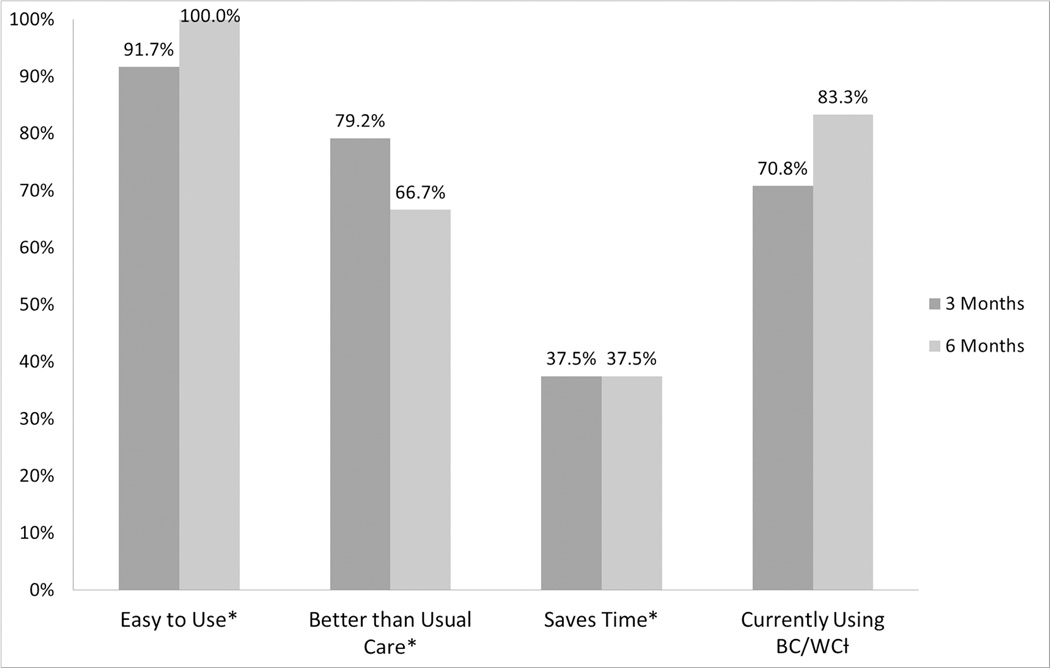
Surgeons completed a median of 10 of 11 BC/WC elements with both standardized and hospitalized patients (range 5-11). We found moderate variability in presentation of treatment options and description of outcomes. Three months after training, 79% of surgeons reported BC/WC is better than their usual approach and 71% endorsed active use of BC/WC in clinical practice. Patients and families found that BC/WC established expectations, provided clarity, and facilitated deliberation.
Surgeons can learn to use BC/WC with older patients considering acute high-risk surgical interventions. Surgeons, patients, and family members endorse BC/WC as a strategy to support complex decision making.
老年人常在死亡前几个月接受手术,这可能引发与临终价值观不一致的术后治疗。“最佳情况/最差情况”(BC/WC)是一种沟通工具,旨在在关于高风险手术的讨论中促进目标一致的护理。
本研究的目的是评估一个结构化培训项目,该项目旨在教导外科医生如何使用BC/WC。
来自一家三级医疗医院的25名外科医生完成了一次两小时的培训课程,随后接受个人辅导。我们对外科医生使用BC/WC与标准化病人及20名住院病人交流的过程进行了录音。住院病人及其家属在入组后30至120天参加了一次开放式访谈。我们使用一份包含11个BC/WC要素的清单来衡量工具的保真度,外科医生完成了从业者意见调查以衡量该工具的可接受性。我们使用定性分析来评估工具内容的变异性,并描述病人及家属对该工具的看法。
外科医生在与标准化病人和住院病人交流时,11个BC/WC要素的中位数完成数为10个(范围为5 - 11)。我们发现治疗方案的呈现和结果的描述存在适度的变异性。培训三个月后,79%的外科医生报告称BC/WC比他们通常的方法更好,71%的人支持在临床实践中积极使用BC/WC。病人和家属发现BC/WC设定了期望,提供了清晰度,并促进了深思熟虑。
对于考虑急性高风险外科干预的老年患者,外科医生可以学会使用BC/WC。外科医生、患者和家属都认可BC/WC作为支持复杂决策的一种策略。