Barba Carmen, Mai Roberto, Grisotto Laura, Gozzo Francesca, Pellacani Simona, Tassi Laura, Francione Stefano, Giordano Flavio, Cardinale Francesco, Guerrini Renzo
Neuroscience Department Children's Hospital Anna Meyer-University of Florence Florence Italy.
"Claudio Munari" Epilepsy Surgery Center Niguarda Hospital Milan Italy.
Ann Clin Transl Neurol. 2016 Nov 19;4(1):36-45. doi: 10.1002/acn3.373. eCollection 2017 Jan.
To assess factors associated with favorable seizure outcome after surgery for symptomatic epileptic spasms and improve knowledge on pathophysiology of this seizure type.
Inclusion criteria were: (1) age between 6 months and 15 years at surgery; (2) active epileptic spasms; (3) follow-up after surgery >1 year.
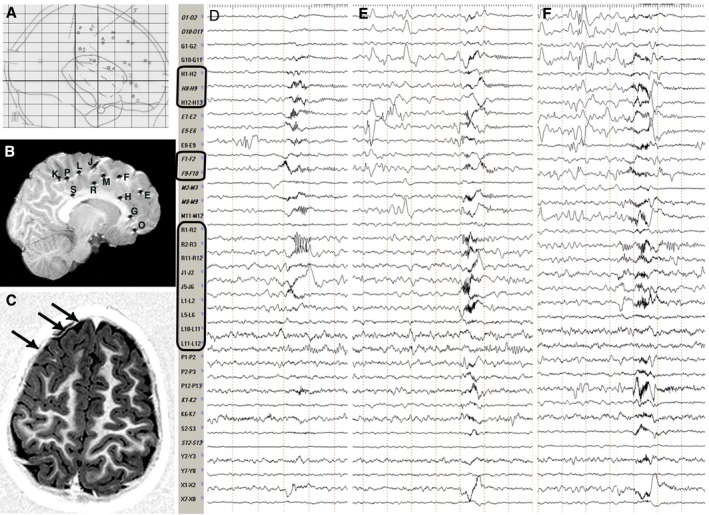
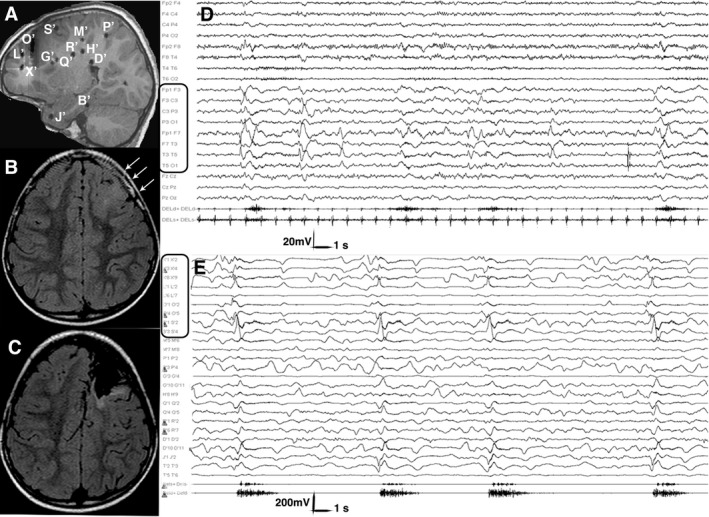
We retrospectively studied 80 children (aged 1.3 ± 2 years at seizure onset; 5.8 ± 4 years at surgery, 11.7 ± 5.7 years at last follow up). Magnetic resonance imaging (MRI) revealed structural abnormalities in 77/80 patients (96.3%; unilateral in 69: 89.6%). We performed invasive recordings in 24 patients (30%). In 21 patients in whom MRI or histopathology detected a lesion, electrodes exploring it constantly captured initial ictal activity at spasm onset. Fifty-eight patients (72.5%) underwent unilobar and 22 (27.5%) multilobar or hemispheric procedures. At last follow-up, 49 patients (61.3%) were in Engel class I. Multivariate logistic models showed completeness of resection of the seizure onset zone (OR = 0.016, 95%CI: 0.002, 0.122) and of the MRI visible lesion (OR = 0.179, 95% CI: 0.032, 0.999) to be significantly associated with Engel class IA outcome. Unfavorable outcome was associated with an older age at surgery, when it reflected a longer duration of epilepsy (OR = 1.383, 95% CI: 0.994,1.926).
Data emerging from invasive recordings and the good seizure outcome following removal of discrete epileptogenic lesions support a focal cortical origin of spasms. In patients with discrete epileptogenic lesions, the pragmatic approach to surgery should follow the same principles applied to focal epilepsy favoring, whenever possible, unilobar, one-stage resections.
评估症状性癫痫性痉挛手术后癫痫发作良好转归的相关因素,并增进对这种癫痫发作类型病理生理学的认识。
纳入标准为:(1)手术时年龄在6个月至15岁之间;(2)有活动性癫痫性痉挛;(3)术后随访>1年。
我们回顾性研究了80名儿童(癫痫发作起始时年龄为1.3±2岁;手术时年龄为5.8±4岁,末次随访时年龄为11.7±5.7岁)。磁共振成像(MRI)显示80例患者中有77例(96.3%)存在结构异常(69例为单侧异常:89.6%)。我们对24例患者(30%)进行了侵入性记录。在MRI或组织病理学检测到病变的21例患者中,探测病变的电极在痉挛发作时持续捕捉到初始发作期活动。58例患者(72.5%)接受了单叶手术,22例(27.5%)接受了多叶或半球手术。在末次随访时,49例患者(61.3%)处于恩格尔I级。多变量逻辑模型显示,癫痫发作起始区的切除完整性(OR=0.016,95%CI:0.002,0.122)和MRI可见病变的切除完整性(OR=0.179,95%CI:0.032,0.999)与恩格尔IA级转归显著相关。不良转归与手术时年龄较大有关,这反映癫痫病程较长(OR=1.383,95%CI:0.994,1.926)。
侵入性记录得出的数据以及切除离散性致痫病变后良好的癫痫发作转归支持痉挛的局灶性皮质起源。对于有离散性致痫病变的患者,手术的务实方法应遵循适用于局灶性癫痫的相同原则,尽可能采用单叶一期切除。