Proietti Marco, Airaksinen K E Juhani, Rubboli Andrea, Schlitt Axel, Kiviniemi Tuomas, Karjalainen Pasi P, Lip Gregory Y H
University of Birmingham Institute of Cardiovascular Sciences, City Hospital, Dudley Road, Birmingham, B18 7QH, UK.
Heart Center, Turku University Hospital and University of Turku, Turku, Finland.
Clin Res Cardiol. 2017 Jun;106(6):420-427. doi: 10.1007/s00392-016-1071-0. Epub 2017 Jan 11.
In patients with atrial fibrillation (AF), quality of oral anticoagulation control as well as impaired renal function are associated with adverse outcomes. Our objective was to analyze if there was a synergistic impact of these factors in determining adverse outcomes in AF patients undergoing percutaneous coronary intervention and stent (PCI-S).
Post-hoc analysis from the Atrial Fibrillation Undergoing Coronary Artery Stenting (AFCAS) registry. Poor oral anticoagulation control was defined as time in therapeutic range (TTR) <65%, while impaired renal function as creatinine clearance (CrCl) <60 ml/min.
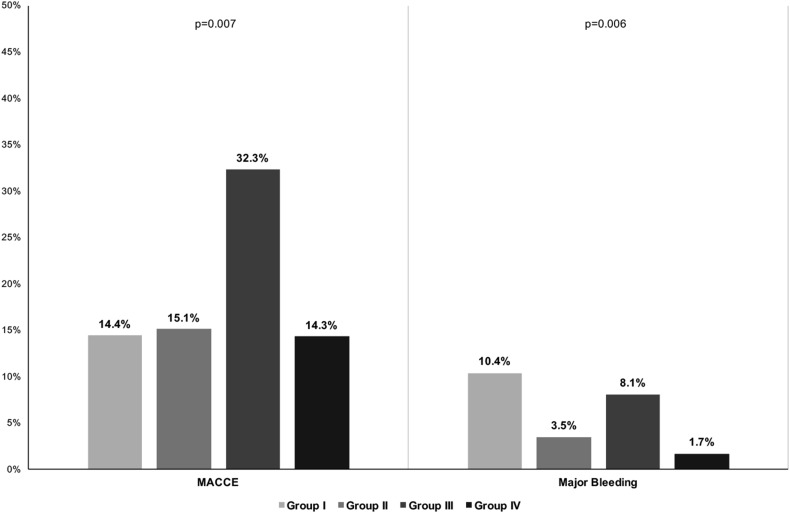
Of the whole cohort, 448 were eligible for this post-hoc analysis. Of these, 27.9% had TTR <65%only (Group I), 19.2% had CrCl <60 ml/min only (Group II), while 13.8% had both conditions (Group III). At follow-up, patients in Group III had a higher rate of major adverse cardiovascular and cerebrovascular events (MACCE) (p = 0.007), while patients in Groups I and III had higher rates of major bleeding. Kaplan-Meier analyses showed that patients in Group III had higher risk for MACCE (LogRank: 14.406, p = 0.003), while Group I and Group III patients had higher risk for major bleeding (LogRank: 12.290, p = 0.006). On Cox regression, presence of both conditions independently increased MACCE risk (p = 0.001), while TTR <65% alone and the presence of both conditions were independently associated with major bleeding (p = 0.004 and p = 0.028, respectively).
There was a synergic impact of oral anticoagulation control and renal function in determining major adverse events in AF patients undergoing PCI-S. Use of poor anticoagulation control and impaired renal function in combination would help identify AF patients undergoing PCI-S at risk for MACCE and/or major bleeding.
在心房颤动(AF)患者中,口服抗凝控制质量以及肾功能受损均与不良结局相关。我们的目的是分析这些因素在接受经皮冠状动脉介入治疗和支架置入术(PCI-S)的AF患者中对不良结局的影响是否具有协同作用。
来自冠状动脉支架置入术中心房颤动(AFCAS)登记处的事后分析。口服抗凝控制不佳定义为治疗范围内时间(TTR)<65%,而肾功能受损定义为肌酐清除率(CrCl)<60 ml/min。
在整个队列中,448例符合此项事后分析的条件。其中,仅27.9%的患者TTR<65%(I组),仅19.2%的患者CrCl<60 ml/min(II组),而13.8%的患者两种情况均存在(III组)。随访时,III组患者发生主要不良心血管和脑血管事件(MACCE)的发生率更高(p = 0.007),而I组和III组患者发生大出血的发生率更高。Kaplan-Meier分析显示,III组患者发生MACCE的风险更高(对数秩检验:14.406,p = 0.003),而I组和III组患者发生大出血的风险更高(对数秩检验:12.290,p = 0.006)。在Cox回归分析中,两种情况同时存在独立增加MACCE风险(p = 0.001),而单独TTR<65%以及两种情况同时存在均与大出血独立相关(分别为p = 0.004和p = 0.028)。
口服抗凝控制和肾功能在决定接受PCI-S的AF患者的主要不良事件方面具有协同作用。联合使用抗凝控制不佳和肾功能受损有助于识别接受PCI-S的AF患者发生MACCE和/或大出血的风险。