Gaduputi Vinaya, Tariq Hassan, Chandrala Chaitanya, Sakam Sailaja, Abbas Naeem, Chilimuri Sridhar
Department of Medicine, Bronx Lebanon Hospital Center, 1650 Selwyn Ave., Suite #10C, Bronx, NY 10457, USA.
J Clin Med Res. 2017 Feb;9(2):92-97. doi: 10.14740/jocmr2832w. Epub 2016 Dec 31.
Ascites remains the most common cause of hospitalization among patients with decompensated cirrhosis. Paracentesis is a relatively safe procedure with low complication rates. Computerized tomography (CT)-guided therapeutic paracentesis could be a safe and effective alternative to unaided or aided (ultrasonogram-guided) bedside paracentesis. In this retrospective study, we aimed to compare the efficacy, safety, and cost-effectiveness of CT-guided paracentesis with bedside paracentesis.
The period of study was from 2002 to 2012. All patients with cirrhosis who underwent therapeutic paracentesis were included in the study. These patients were divided into two groups. Group I consisted of patients who underwent CT-guided pigtail catheter insertion with ascitic fluid drainage. Group II consisted of patients who underwent beside therapeutic paracentesis after localization of fluid either by physical examination or sonographic localization. We measured the efficacy of CT-guided paracentesis and bedside paracentesis in terms of volume of fluid removed, length of stay, discharge doses of diuretics (spironolactone and furosemide) and number of days to readmission for symptomatic ascites. We also computed the cost-effectiveness of CT-guided therapeutic paracentesis when compared to a bedside procedure. Fischer exact test was used to analyze the distribution of categorical data and unpaired -test was used for comparison of means.
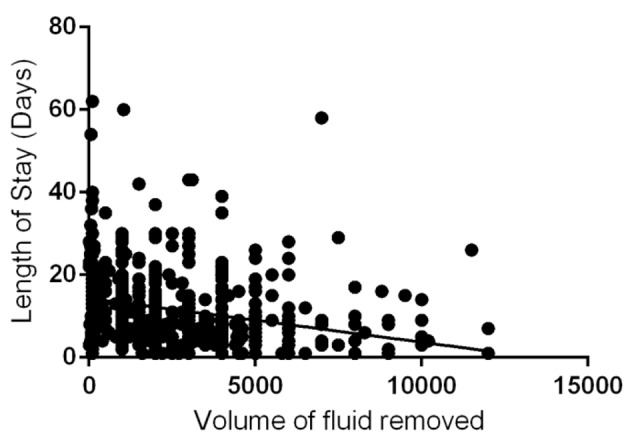
There were a total of 546 unique patients with diagnosed cirrhosis who were admitted to the hospital with symptomatic ascites and underwent therapeutic paracentesis. Two hundred and forty-seven patients underwent CT-guided paracentesis, while 272 patients underwent bedside paracentesis. There was significant inverse correlation between the amount of ascitic fluid removed and total length of stay in the hospital. We found that the volume of fluid removed via a CT-guided pigtail insertion and drainage (2.72 ± 2.02 L) is significantly higher when compared to fluid removed via bedside paracentesis (1.94 ± 1.69). We also found that the interval time period between two successive therapeutic paracenteses was significantly longer for CT group (106.56 ± 75.2 days) when compared to the bedside group (25.57 ± 7.68 days).
CT-guided paracentesis with pigtail catheter insertion and drainage is a clinically effective, cheap and safe alternative to conventional bedside paracentesis.
腹水仍然是失代偿期肝硬化患者住院治疗最常见的原因。腹腔穿刺术是一种相对安全的操作,并发症发生率较低。计算机断层扫描(CT)引导下的治疗性腹腔穿刺术可能是徒手或辅助(超声引导)床边腹腔穿刺术的一种安全有效的替代方法。在这项回顾性研究中,我们旨在比较CT引导下腹腔穿刺术与床边腹腔穿刺术的疗效、安全性和成本效益。
研究时间段为2002年至2012年。所有接受治疗性腹腔穿刺术的肝硬化患者均纳入研究。这些患者被分为两组。第一组由接受CT引导下猪尾导管置入并引流腹水的患者组成。第二组由通过体格检查或超声定位确定腹水位置后在床边进行治疗性腹腔穿刺术的患者组成。我们从腹水排出量、住院时间、出院时利尿剂(螺内酯和呋塞米)剂量以及因症状性腹水再次入院的天数方面来衡量CT引导下腹腔穿刺术和床边腹腔穿刺术的疗效。我们还计算了与床边操作相比CT引导下治疗性腹腔穿刺术的成本效益。采用Fisher精确检验分析分类数据的分布情况,采用非配对t检验比较均值。
共有546例确诊肝硬化且因症状性腹水入院并接受治疗性腹腔穿刺术的患者。247例患者接受了CT引导下腹腔穿刺术,272例患者接受了床边腹腔穿刺术。腹水排出量与住院总时长之间存在显著的负相关关系。我们发现,与床边腹腔穿刺术排出的腹水量(1.94±1.69L)相比,通过CT引导下猪尾导管置入并引流排出的腹水量(2.72±2.02L)显著更高。我们还发现,与床边组(25.57±7.68天)相比,CT组两次连续治疗性腹腔穿刺术之间的间隔时间显著更长(106.56±75.2天)。
CT引导下猪尾导管置入并引流的腹腔穿刺术是传统床边腹腔穿刺术的一种临床有效、廉价且安全的替代方法。