Cozijnsen M A, van Pieterson M, Samsom J N, Escher J C, de Ridder L
Department of Paediatric Gastroenterology , Erasmus University Medical Centre-Sophia Children's Hospital , Rotterdam , The Netherlands.
Laboratory of Paediatrics , Erasmus University Medical Centre-Sophia Children's Hospital , Rotterdam , The Netherlands.
BMJ Open Gastroenterol. 2016 Dec 22;3(1):e000123. doi: 10.1136/bmjgast-2016-000123. eCollection 2016.
Crohn's disease (CD) is a chronic inflammatory disease predominantly affecting the gastrointestinal tract. CD usually requires lifelong medication and is accompanied by severe complications, such as fistulae and strictures, resulting in surgery. Infliximab (IFX) is very effective for treating paediatric patients with CD, but is currently only registered for therapy refractory patients-the so-called step-up strategy. We hypothesise that using IFX first-line, that is, top-down, will give more mucosal healing, fewer relapses, less complications, need for surgery and hospitalisation.
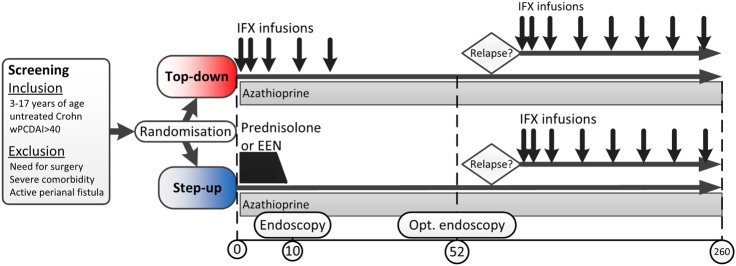
This international multicentre open-label randomised controlled trial includes children, aged 3-17 years, with new-onset, untreated CD with moderate-to-severe disease activity (weighted Paediatric Crohn's Disease Activity Index (wPCDAI)>40). Eligible patients will be randomised to top-down or step-up treatment. Top-down treatment consists of 5 IFX infusions combined with azathioprine (AZA). After these 5 infusions, patients will continue AZA. Patients randomised to step-up will receive standard induction treatment, either oral prednisolone or exclusive enteral nutrition, combined with AZA as maintenance treatment. The primary outcome is clinical remission (wPCDAI<12.5) at 52 weeks without need for additional CD-related therapy or surgery. Total follow-up is 5 years. Secondary outcomes include clinical disease activity, mucosal healing by endoscopy (at week 10 and optionally week 52), faecal calprotectin, growth, quality of life, medication use and adverse events.
Conducted according to the Declaration of Helsinki and Good Clinical Practice. Medical-ethical approval will be obtained for each site.
NCT02517684; Pre-results.
克罗恩病(CD)是一种主要影响胃肠道的慢性炎症性疾病。CD通常需要终身药物治疗,并伴有严重并发症,如瘘管和狭窄,最终可能需要手术。英夫利昔单抗(IFX)对治疗儿童CD患者非常有效,但目前仅获批用于治疗难治性患者,即所谓的逐步升级策略。我们假设一线使用IFX,即自上而下的治疗方法,将带来更多的黏膜愈合、更少的复发、更少的并发症、手术需求和住院次数。
这项国际多中心开放标签随机对照试验纳入了3至17岁新诊断、未经治疗且疾病活动度为中度至重度(加权儿科克罗恩病活动指数(wPCDAI)>40)的CD患儿。符合条件的患者将被随机分配至自上而下或逐步升级治疗组。自上而下治疗包括5次IFX输注联合硫唑嘌呤(AZA)。这5次输注后,患者将继续使用AZA。随机分配至逐步升级治疗组的患者将接受标准诱导治疗,即口服泼尼松龙或全肠内营养,并联合AZA作为维持治疗。主要结局是52周时临床缓解(wPCDAI<12.5),且无需额外的CD相关治疗或手术。总随访时间为5年。次要结局包括临床疾病活动度、内镜检查的黏膜愈合情况(第10周,可选第52周)、粪便钙卫蛋白、生长发育、生活质量、药物使用情况及不良事件。
按照《赫尔辛基宣言》和《药物临床试验质量管理规范》进行。每个研究地点都将获得医学伦理批准。
NCT02517684;预结果。