Department of Pediatric Gastroenterology, Erasmus Medical Centre-Sophia Children's Hospital, Room SP-2430, P.O. Box 2040, 3000, Rotterdam, CA, Netherlands.
Department of Pediatric Gastroenterology, Isala Hospital, Zwolle, Netherlands.
Eur J Pediatr. 2022 Aug;181(8):3055-3065. doi: 10.1007/s00431-022-04496-7. Epub 2022 Jun 8.
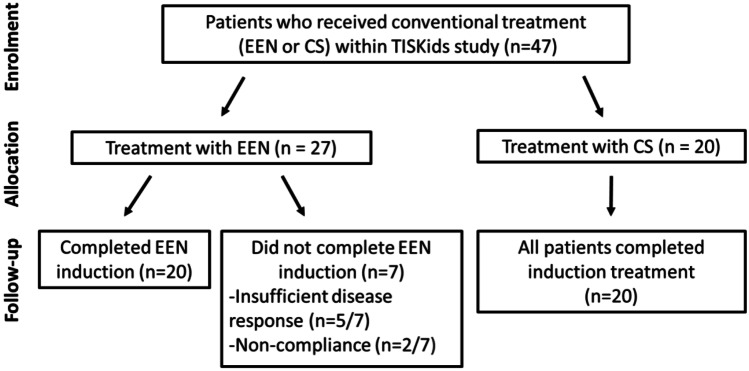
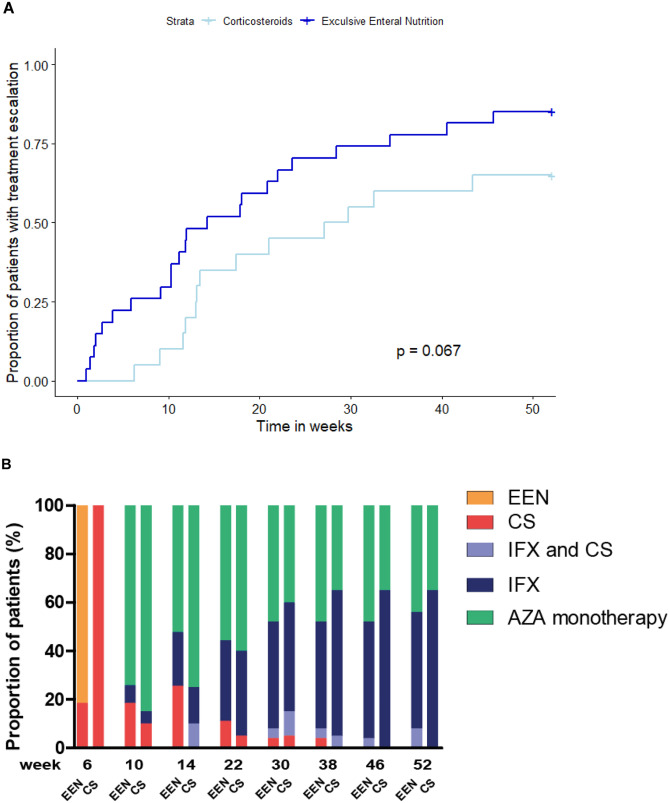
To induce remission in luminal paediatric Crohn's disease (CD), the ESPGHAN/ECCO guideline recommends treatment with exclusive enteral nutrition (EEN) or oral corticosteroids. In newly diagnosed moderate-to-severe paediatric CD patients, we determined the proportion of patients in which EEN or corticosteroids induced remission and maintained remission on azathioprine monotherapy. We included patients from the "TISKids" study assigned to the conventional treatment arm. Patients were aged 3-17 years and had new-onset, untreated luminal CD with weighted paediatric CD activity index (wPCDAI) > 40. Induction treatment consisted of EEN or oral corticosteroids; all received azathioprine maintenance treatment from start of treatment. The primary outcome of this study was endoscopic remission defined as a SES-CD score < 3 without treatment escalation at week 10. Secondary outcomes included proportion of patients without treatment escalation at week 52. In total, 27/47 patients received EEN and 20/47 corticosteroids. At baseline, patient demographics and several inflammation parameters were similar between the two treatment groups. At 10 weeks, clinical remission rates were 7/23 (30%) for EEN and 7/19 (37%) for corticosteroids (p = 0.661). Twenty-nine of 47 consented to endoscopy at 10 weeks, showing endoscopic remission rates without treatment escalation in 2/16 (13%) of EEN-treated patients and in 1/13 (8%) of corticosteroid-treated patients (p = 1.00). At week 52, 23/27 (85%) EEN-treated patients received treatment escalation (median 14 weeks) and 13/20 (65%) corticosteroid-treated patients (median 27 weeks), p = 0.070.Conclusion: In children with moderate-to-severe newly diagnosed CD, induction treatment with EEN or CS regularly is insufficient to achieve endoscopic remission without treatment escalation at week 10. Trial registration number: NCT02517684 What is Known: • Endoscopic remission is associated with a low risk of disease progression. • FL-IFX was superior to conventional treatment in achieving and maintaining remission in paediatric patients with moderate-to-severe CD the first year from diagnosis. What is New: • In children with newly diagnosed moderate-to-severe CD, clinical remission rates and endoscopic remission rates without treatment escalation at week 10 were 30% and 13% after EEN and 37% and 8% after corticosteroid induction treatment. • The current treatment target was often not achieved by either EEN or corticosteroid induction treatment after bridging to azathioprine.
在诱导儿科克罗恩病(CD)缓解方面,ESPGHAN/ECCO 指南推荐使用肠内营养(EEN)或口服皮质类固醇治疗。在新诊断的中重度儿科 CD 患者中,我们确定了 EEN 或皮质类固醇诱导缓解并在硫唑嘌呤单药治疗下维持缓解的患者比例。我们纳入了来自“TISKids”研究的被分配到常规治疗组的患者。患者年龄为 3-17 岁,新发、未经治疗的腔型 CD,加权儿科 CD 活动指数(wPCDAI)>40。诱导治疗包括 EEN 或口服皮质类固醇;所有患者从治疗开始时都接受硫唑嘌呤维持治疗。本研究的主要结局是内镜缓解,定义为 SES-CD 评分<3,且在第 10 周时未进行治疗升级。次要结局包括第 52 周时未进行治疗升级的患者比例。总共有 27/47 例患者接受 EEN,20/47 例患者接受皮质类固醇治疗。在基线时,两组患者的人口统计学特征和几项炎症参数相似。在第 10 周时,EEN 的临床缓解率为 7/23(30%),皮质类固醇的缓解率为 7/19(37%)(p=0.661)。在第 10 周时,47 名患者中有 29 名同意进行内镜检查,EEN 治疗组有 2/16(13%)的患者和皮质类固醇治疗组有 1/13(8%)的患者(p=1.00)未进行治疗升级,内镜缓解率无显著差异。在第 52 周时,27/27(85%)EEN 治疗组患者需要进行治疗升级(中位时间为 14 周),20/20(65%)皮质类固醇治疗组患者需要进行治疗升级(中位时间为 27 周)(p=0.070)。结论:在新诊断为中重度的儿童 CD 患者中,EEN 或 CS 诱导治疗通常不足以在第 10 周时实现内镜缓解,且无需进行治疗升级。研究注册号:NCT02517684 已知内容:•内镜缓解与疾病进展风险低相关。•FL-IFX 在诱导缓解和维持缓解方面优于传统治疗,可用于治疗第一年新诊断为中重度 CD 的儿科患者。新内容:•在新诊断为中重度 CD 的儿童中,EEN 或皮质类固醇诱导治疗后第 10 周的临床缓解率和内镜缓解率(无治疗升级)分别为 30%和 13%,而皮质类固醇诱导治疗后的缓解率分别为 37%和 8%。•EEN 或皮质类固醇诱导治疗后,大多数患者都需要桥接至硫唑嘌呤治疗。