Liu Jian-Ye, Dai Ying-Bo, Zhou Fang-Jian, Long Zhi, Li Yong-Hong, Xie Dan, Liu Bin, Tang Jin, Tan Jing, Yao Kun, He Le-Ye
Department of Urology, The Third Xiangya Hospital of Central South University, No.138, Tongzipo Road, Changsha, 410013, Hunan, China.
Institute of Prostate Disease of Central South University, No.138, Tongzipo Road, Changsha, 410013, Hunan, China.
BMC Surg. 2017 Jan 17;17(1):8. doi: 10.1186/s12893-016-0202-x.
Many studies have reported the oncological outcomes between open radical nephroureterectomy (ONU) and laparoscopic radical nephroureterectomy (LNU) of upper tract urothelial carcinoma (UTUC). However, few data have focused on the oncological outcomes of LNU in the subgroup of localized and/or locally advanced UTUC (T/N). The purpose of this study was to compare the oncological outcomes of LNU vs. ONU for the treatment in patients with T/N UTUC.
We collected and analyzed the data and clinical outcomes retrospectively for 265 patients who underwent radical nephroureterectomy for T/N UTUC between April 2000 and April 2013 at two Chinese tertiary hospitals. Survival was estimated using the Kaplan-Meier method. Cox's proportional hazards model was used for univariate and multivariate analysis.
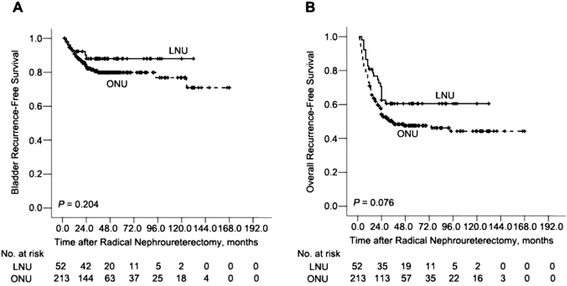
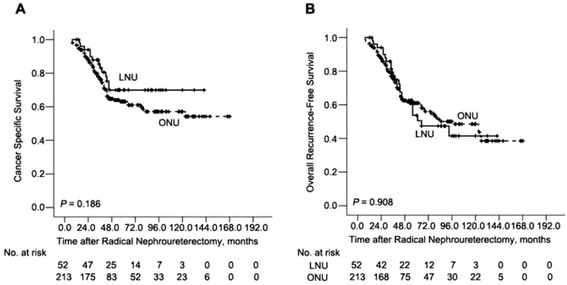
The mean patient age was 62.0 years and the median follow-up was 60.0 months. Of the 265 patients, 213 (80.4%) underwent conventional ONU, and 52 (19.6%) patients underwent LNU. The groups differed significantly in their presence of previous hydronephrosis, presence of previous bladder urothelial carcinoma, and management of distal ureter (P < 0.05). The predicted 5-year intravesical recurrence- free survival (RFS) (79% vs. 88%, P = 0.204), overall RFS (47% vs. 59%, P = 0.076), cancer-specific survival (CSS) (63% vs. 70%, P = 0.186), and overall survival (OS) (61% vs. 55%, P = 0.908) rates did not differ between the ONU and LNU groups. Multivariable Cox proportional regression analysis showed that surgical approach was not significantly associated with intravesical RFS (odds ratio [OR] 1.23, 95% confidence interval [CI] 0.46-3.65, P = 0.622), Overall RFS (OR 0.99, 95% CI 0.54-1.83, P = 0.974), CSS (OR 1.38, 95% CI 0.616-3.13, P = 0.444), or OS (OR 1.61, 95% CI 0.81-3.17, P = 0.17).
The results of this retrospective study showed no statistically significant differences in intravesical RFS, overall RFS, CSS, or OS between the laparoscopy and the open groups. Thus, LNU can be an alternative to the open procedure for T/N UTUC. Further studies, including a multi-institutional, prospective study are required to confirm these findings.
许多研究报告了开放性根治性肾输尿管切除术(ONU)与腹腔镜根治性肾输尿管切除术(LNU)治疗上尿路尿路上皮癌(UTUC)的肿瘤学结局。然而,很少有数据关注LNU在局限性和/或局部进展性UTUC(T/N)亚组中的肿瘤学结局。本研究的目的是比较LNU与ONU治疗T/N UTUC患者的肿瘤学结局。
我们回顾性收集并分析了2000年4月至2013年4月期间在中国两家三级医院接受T/N UTUC根治性肾输尿管切除术的265例患者的数据和临床结局。采用Kaplan-Meier法估计生存率。Cox比例风险模型用于单因素和多因素分析。
患者平均年龄为62.0岁,中位随访时间为60.0个月。265例患者中,213例(80.4%)接受了传统ONU,52例(19.6%)患者接受了LNU。两组在既往肾积水、既往膀胱尿路上皮癌的存在以及输尿管远端的处理方面存在显著差异(P<0.05)。ONU组和LNU组的预测5年膀胱内无复发生存率(RFS)(79%对88%,P=0.204)、总体RFS(47%对59%,P=0.076)、癌症特异性生存率(CSS)(63%对70%,P=0.186)和总生存率(OS)(61%对55%,P=0.908)无差异。多变量Cox比例回归分析显示,手术方式与膀胱内RFS(优势比[OR]1.23,95%置信区间[CI]0.46-3.65,P=0.622)、总体RFS(OR 0.99,95%CI 0.54-1.83,P=0.974)、CSS(OR 1.38,95%CI 0.616-3.13,P=0.444)或OS(OR 1.61,95%CI 0.81-3.17,P=0.17)无显著相关性。
这项回顾性研究的结果显示,腹腔镜组和开放手术组在膀胱内RFS、总体RFS、CSS或OS方面无统计学显著差异。因此,对于T/N UTUC,LNU可作为开放手术的替代方案。需要进一步的研究,包括多机构前瞻性研究来证实这些发现。