Talwar Nidhi, Musch David C, Stein Joshua D
Department of Ophthalmology and Visual Sciences, University of Michigan Medical School, Ann Arbor2Center for Eye Policy and Innovation, University of Michigan, Ann Arbor.
Department of Ophthalmology and Visual Sciences, University of Michigan Medical School, Ann Arbor2Center for Eye Policy and Innovation, University of Michigan, Ann Arbor3Department of Epidemiology, University of Michigan School of Public Health, Ann Arbor.
JAMA Ophthalmol. 2017 Mar 1;135(3):263-267. doi: 10.1001/jamaophthalmol.2016.5406.
There is growing evidence that statins may protect against the development or worsening of open-angle glaucoma (OAG). As researchers plan clinical trials to more definitively study whether statins indeed protect against OAG, it would be helpful to know whether specific daily dosages or types of statin confer a greater protective effect than others.
To assess whether the protective effect of statins on the risk of glaucoma varies depending on the daily dosage or type of statin taken.
DESIGN, SETTING, AND PARTICIPANTS: Using claims data from January 2001 to December 2009, we observed 25 420 patients with no preexisting glaucoma and quantified exposure to statins and other cholesterol-lowering medications. Using multivariable regression modeling, we assessed the hazard of developing OAG and how it varied by the daily dosage or type of statin and whether any protective effect persists after accounting for baseline low-density lipoprotein level.
Different daily dosages and types of statins.
Hazard ratios (HRs) for developing OAG with 95% CIs.
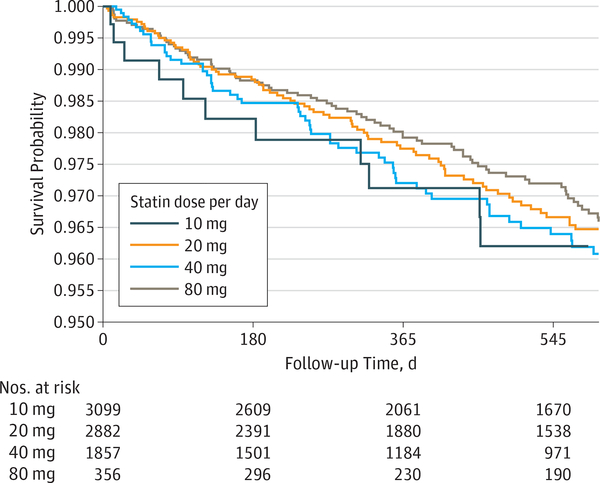
Of the 25 420 patients who met the eligibility criteria for study inclusion, the mean (SD) age was 66.1 (5.8) years, and 14 112 (55.5%) were female. Additionally, 19 232 patients (84.1%) were white, 1252 (5.5%) were black, and 1558 (6.8%) were Latino. After accounting for baseline low-density lipoprotein levels, persons who filled prescriptions for statins continuously for 2 years had a 21% reduced risk of glaucoma compared with nonusers (adjusted HR, 0.79; 95% CI, 0.66-0.96; P = .02). There was no additional protective effect associated with taking the highest dosage of statins (80 mg) compared with a lower dosage (40 mg) (HR, 1.03; 95% CI, 0.59-1.80; P = .91). The protective effect of the following statins on OAG risk did not differ compared with atorvastatin, an inexpensive generic statin: lovastatin (HR, 1.09; 95% CI, 0.71-1.68; P = .69), cerivastatin (HR, 0.61; 95% CI, 0.09-4.41; P = .63), rosuvastatin (HR, 0.83; 95% CI, 0.48-1.44; P = .51), fluvastatin (HR, 0.89; 95% CI, 0.39-2.02; P = .78), pravastatin (HR, 1.29; 95% CI, 0.93-1.79; P = .13), and simvastatin (HR, 1.03; 95% CI, 0.83-1.29; P = .78).
Even after accounting for baseline low-density lipoprotein level, statin exposure continued to be associated with a reduction in OAG risk. Our study helps inform researchers of a reasonable daily dosage and type of statin to use when designing randomized clinical trials to assess the association between statin use and glaucoma.
越来越多的证据表明,他汀类药物可能预防开角型青光眼(OAG)的发生或病情恶化。随着研究人员计划开展临床试验以更明确地研究他汀类药物是否真的能预防OAG,了解特定的每日剂量或他汀类药物类型是否比其他药物具有更强的保护作用将有所帮助。
评估他汀类药物对青光眼风险的保护作用是否因所服用的他汀类药物的每日剂量或类型而异。
设计、设置和参与者:利用2001年1月至2009年12月的索赔数据,我们观察了25420例既往无青光眼的患者,并对他汀类药物和其他降胆固醇药物的暴露情况进行了量化。我们使用多变量回归模型评估发生OAG的风险,以及该风险如何因他汀类药物的每日剂量或类型而变化,以及在考虑基线低密度脂蛋白水平后是否仍存在任何保护作用。
不同的每日剂量和他汀类药物类型。
发生OAG的风险比(HRs)及95%可信区间(CIs)。
在符合研究纳入资格标准的25420例患者中,平均(标准差)年龄为66.1(5.8)岁,女性有14112例(55.5%)。此外,19232例患者(84.1%)为白人,1252例(5.5%)为黑人,1558例(6.8%)为拉丁裔。在考虑基线低密度脂蛋白水平后,连续2年服用他汀类药物处方的患者与未使用者相比,患青光眼的风险降低了21%(调整后的HR为0.79;95%CI为0.66-0.96;P = 0.02)。与较低剂量(40mg)相比,服用最高剂量他汀类药物(80mg)没有额外的保护作用(HR为1.03;95%CI为0.59-1.80;P = 0.91)。与阿托伐他汀(一种廉价的非专利他汀类药物)相比,以下他汀类药物对OAG风险的保护作用没有差异:洛伐他汀(HR为1.09;95%CI为0.71-1.68;P = 0.69)、西立伐他汀(HR为0.61;95%CI为0.09-4.41;P = 0.63)、瑞舒伐他汀(HR为0.83;95%CI为0.48-1.44;P = 0.51)、氟伐他汀(HR为0.89;95%CI为0.39-2.02;P = 0.78)、普伐他汀(HR为1.29;95%CI为0.93-1.79;P = 0.13)和辛伐他汀(HR为1.03;95%CI为0.83-1.29;P = 0.78)。
即使在考虑基线低密度脂蛋白水平后,他汀类药物暴露仍与OAG风险降低相关。我们的研究有助于为研究人员在设计随机临床试验以评估他汀类药物使用与青光眼之间的关联时,提供关于合理的每日剂量和他汀类药物类型的信息。