Sager Ramon, Kutz Alexander, Mueller Beat, Schuetz Philipp
University Department of Medicine, Kantonsspital Aarau, Tellstrasse, CH-5001, Aarau, Switzerland.
Faculty of Medicine, University of Basel, Basel, Switzerland.
BMC Med. 2017 Jan 24;15(1):15. doi: 10.1186/s12916-017-0795-7.
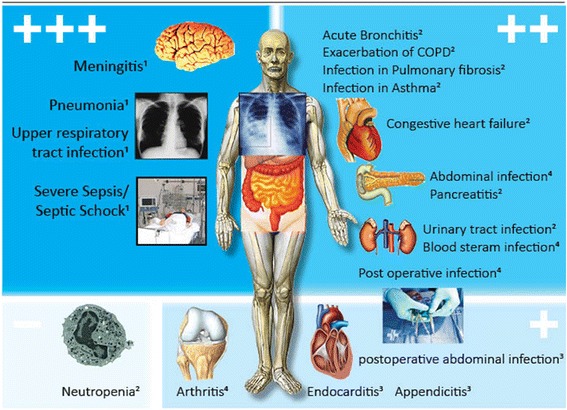
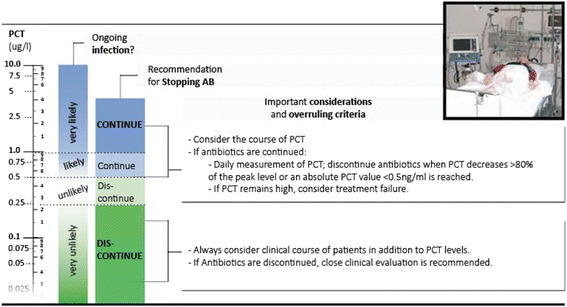
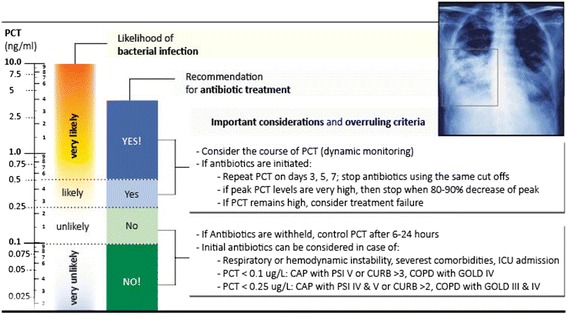
Several controlled clinical studies have evaluated the potential of the infection biomarker procalcitonin (PCT) to improve the diagnostic work-up of patients with bacterial infections and its influence on decisions regarding antibiotic therapy. Most research has focused on lower respiratory tract infections and critically ill sepsis patients. A clinical utility for PCT has also been found for patients with urinary tract infections, postoperative infections, meningitis, and patients with acute heart failure with possible superinfection (i.e., pneumonia). In these indications, PCT levels measured on hospital admission were found to substantially reduce the initiation of antibiotic treatment in low-risk situations (i.e., bronchitis, chronic obstructive pulmonary disease exacerbation). For more severe infections (i.e., pneumonia, sepsis), antibiotic stewardship by monitoring of PCT kinetics resulted in shorter antibiotic treatment durations with early cessation of therapy. Importantly, these strategies appear to be safe without increasing the risk for mortality, recurrent infections, or treatment failures. PCT kinetics also proved to have prognostic value correlating with disease severity (i.e., pancreatitis, abdominal infection) and resolution of illness (i.e., sepsis). Although promising findings have been published in these different types of infections, there are a number of limitations regarding PCT, including suboptimal sensitivity and/or specificity, which makes a careful interpretation of PCT in the clinical context mandatory. This narrative review aims to update clinicians on the strengths and limitations of PCT for patient management, focusing on research conducted within the last 4 years.
多项对照临床研究评估了感染生物标志物降钙素原(PCT)在改善细菌感染患者诊断检查方面的潜力及其对抗生素治疗决策的影响。大多数研究集中在下呼吸道感染和重症脓毒症患者。对于尿路感染、术后感染、脑膜炎以及可能合并二重感染(即肺炎)的急性心力衰竭患者,也发现了PCT的临床应用价值。在这些适应症中,入院时测得的PCT水平在低风险情况下(即支气管炎、慢性阻塞性肺疾病急性加重)可大幅减少抗生素治疗的启动。对于更严重的感染(即肺炎、脓毒症),通过监测PCT动态变化进行抗生素管理可缩短抗生素治疗疗程并提前停止治疗。重要的是,这些策略似乎是安全的,不会增加死亡率、反复感染或治疗失败的风险。PCT动态变化也被证明与疾病严重程度(即胰腺炎、腹腔感染)和疾病缓解情况(即脓毒症)相关,具有预后价值。尽管在这些不同类型的感染中已发表了一些有前景的研究结果,但PCT存在一些局限性,包括敏感性和/或特异性欠佳,这使得在临床背景下对PCT进行仔细解读成为必要。本叙述性综述旨在向临床医生介绍PCT在患者管理方面的优势和局限性,重点关注过去4年开展的研究。