Kakareko Katarzyna, Rydzewska-Rosolowska Alicja, Brzosko Szymon, Gozdzikiewicz-Lapinska Joanna, Koc-Zorawska Ewa, Samocik Pawel, Kozlowski Robert, Mysliwiec Michal, Naumnik Beata, Hryszko Tomasz
I Department of Nephrology and Transplantation with Dialysis Unit, Medical University of Bialystok, Ul. Zurawia 14, 15-540, Białystok, Poland.
II Department of Nephrology and Hypertension with Dialysis Unit, Medical University of Bialystok, Białystok, Poland.
Int Urol Nephrol. 2017 Apr;49(4):681-688. doi: 10.1007/s11255-017-1519-9. Epub 2017 Jan 27.
Increased concentration of fibroblast growth factor 23 (FGF-23) and decreased levels of soluble Klotho (sKL) are linked to negative clinical outcomes among patients with chronic kidney disease and acute kidney injury. Therefore, it is reasonable to hypothesize that GFR reduction caused by nephrectomy might alter mineral metabolism and induces adverse consequences. Whether nephrectomy due to urological indications causes derangements in FGF-23 and sKL has not been studied. The aim of the study was to evaluate the effect of acute GFR decline due to unilateral nephrectomy on bone metabolism, FGF-23 and sKL levels.
This is a prospective, single-centre observational study of patients undergoing nephrectomy due to urological indications. Levels of C-terminal FGF-23 (c-FGF-23), sKL and bone turnover markers [β-crosslaps (CTX), bone-specific alkaline phosphatase (bALP) and tartrate-resistant acid phosphatase 5b (TRAP 5b)] were measured before and after surgery (5 ± 2 days).
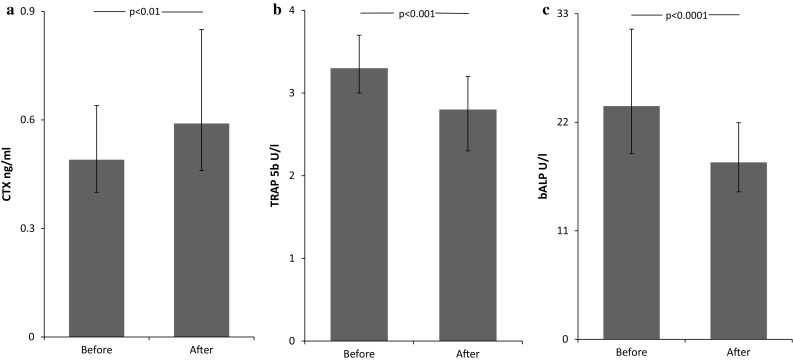
Twenty-nine patients were studied (14 females, age 63.0 ± 11.6, eGFR 87.3 ± 19.2 ml/min/1.73 m). After surgery, eGFR significantly declined (p < 0.0001). Nephrectomy significantly decreased sKL level [709.8 (599.9-831.2) vs. 583.0 (411.7-752.6) pg/ml, p < 0.001] and did not change c-FGF-23 concentration [70.5 (49.8-103.3) vs. 77.1 (60.5-109.1) RU/ml, p = 0.9]. Simultaneously, alterations in bone turnover markers were observed. Serum concentration of CTX increased [0.49 (0.4-0.64) vs. 0.59 (0.46-0.85) ng/ml, p = 0.001], while bALP and TRAP 5b decreased [23.6 (18.8-31.4) vs. 17.9 (15.0-22.0) U/l, p < 0.0001 and 3.3 (3.0-3.7) vs. 2.8 (2.3-3.2) U/l, p < 0.001, respectively].
Nephrectomy among patients with preserved renal function before surgery does not increase c-FGF-23 but reduces sKL. Moreover, nephrectomy results in derangements in bone turnover markers in short-term follow-up. These changes may participate in pathogenesis of bone disease after nephrectomy.
成纤维细胞生长因子23(FGF - 23)浓度升高和可溶性Klotho(sKL)水平降低与慢性肾脏病和急性肾损伤患者的不良临床结局相关。因此,推测肾切除术导致的肾小球滤过率(GFR)降低可能会改变矿物质代谢并引发不良后果是合理的。因泌尿外科指征进行的肾切除术是否会导致FGF - 23和sKL紊乱尚未得到研究。本研究的目的是评估因单侧肾切除术导致的急性GFR下降对骨代谢、FGF - 23和sKL水平的影响。
这是一项对因泌尿外科指征接受肾切除术患者的前瞻性单中心观察性研究。在手术前后(5±2天)测量C末端FGF - 23(c - FGF - 23)、sKL和骨转换标志物[β - 交联C端肽(CTX)、骨特异性碱性磷酸酶(bALP)和抗酒石酸酸性磷酸酶5b(TRAP 5b)]的水平。
研究了29例患者(14例女性,年龄63.0±11.6岁,估算肾小球滤过率[eGFR]87.3±19.2 ml/min/1.73m²)。术后,eGFR显著下降(p<0.0001)。肾切除术使sKL水平显著降低[709.8(599.9 - 831.2)与583.0(411.7 - 752.6)pg/ml,p<0.001],而c - FGF - 23浓度未改变[70.5(49.8 - 103.3)与77.1(60.5 - 109.1)RU/ml,p = 0.9]。同时,观察到骨转换标志物的变化。血清CTX浓度升高[0.49(0.4 - 0.64)与0.59(0.46 - 0.85)ng/ml,p = 0.001],而bALP和TRAP 5b降低[23.6(18.8 - 31.4)与17.9(15.0 - 22.0)U/L,p<0.0001;3.3(3.0 - 3.7)与2.8(2.3 - 3.2)U/L,p<分别为0.001]。
术前肾功能正常的患者进行肾切除术不会增加c - FGF - 23,但会降低sKL。此外,肾切除术在短期随访中导致骨转换标志物紊乱。这些变化可能参与肾切除术后骨病的发病机制。