Wolf H T, Huusom L, Weber T, Piedvache A, Schmidt S, Norman M, Zeitlin J
Department of Obstetrics and Gynaecology, Hvidovre Hospital, Copenhagen University Hospital, Denmark.
Inserm UMR 1153, Obstetrical, Perinatal and Pediatric Epidemiology Research Team (Epopé), Center for Epidemiology and Statistics Sorbonne Paris Cité, DHU Risks in pregnancy, Paris Descartes University, Paris, France.
BMJ Open. 2017 Jan 27;7(1):e013952. doi: 10.1136/bmjopen-2016-013952.
The use of magnesium sulfate (MgSO) in European obstetric units is unknown. We aimed to describe reported policies and actual use of MgSO in women delivering before 32 weeks of gestation by indication.
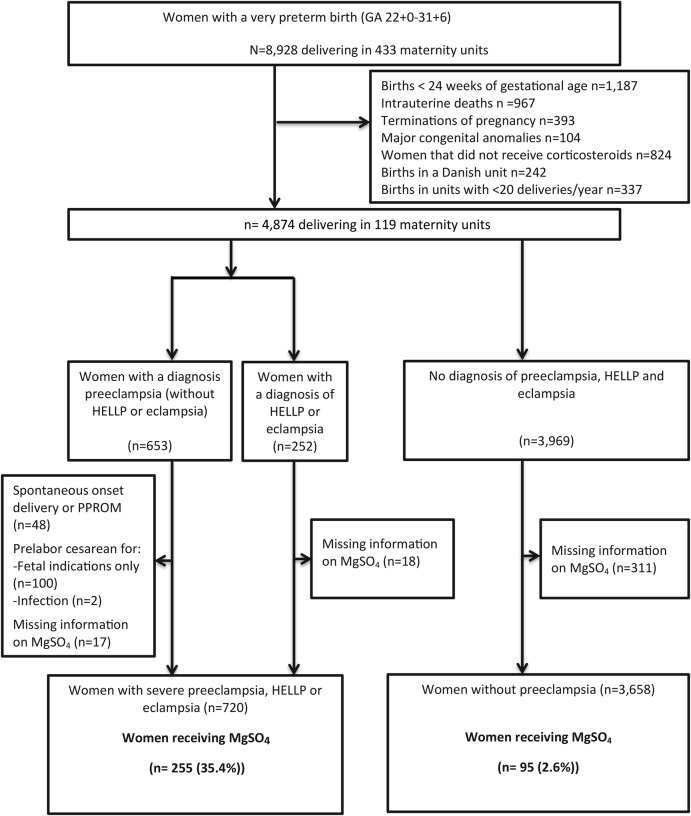
We used data from the European Perinatal Intensive Care in Europe (EPICE) population-based cohort study of births before 32 weeks of gestation in 19 regions in 11 European countries. Data were collected from April 2011 to September 2012 from medical records and questionnaires. The study population comprised 720 women with severe pre-eclampsia, eclampsia or HELLP and 3658 without pre-eclampsia delivering from 24 to 31 weeks of gestation in 119 maternity units with 20 or more very preterm deliveries per year.
Among women with severe pre-eclampsia, eclampsia or HELLP, 255 (35.4%) received MgSO before delivery. 41% of units reported use of MgSO whenever possible for pre-eclampsia and administered MgSO more often than units reporting use sometimes. In women without pre-eclampsia, 95 (2.6%) received MgSO. 9 units (7.6%) reported using MgSO for fetal neuroprotection whenever possible. In these units, the median rate of MgSO use for deliveries without severe pre-eclampsia, eclampsia and HELLP was 14.3%. Only 1 unit reported using MgSO as a first-line tocolytic. Among women without pre-eclampsia, MgSO use was not higher in women hospitalised before delivery for preterm labour.
Severe pre-eclampsia, eclampsia or HELLP are not treated with MgSO as frequently as evidence-based medicine recommends. MgSO is seldom used for fetal neuroprotection, and is no longer used for tocolysis. To continuously lower morbidity, greater attention to use of MgSO is needed.
硫酸镁(MgSO)在欧洲产科病房的使用情况尚不清楚。我们旨在按指征描述妊娠32周前分娩的女性中硫酸镁的报告政策和实际使用情况。
我们使用了欧洲围产期重症监护(EPICE)基于人群的队列研究数据,该研究涉及11个欧洲国家19个地区妊娠32周前的出生情况。数据于2011年4月至2012年9月从病历和问卷中收集。研究人群包括720例患有重度子痫前期、子痫或HELLP综合征的女性以及3658例无子痫前期的女性,她们在每年有20次或更多极早产分娩的119个产科病房中于妊娠24至31周分娩。
在患有重度子痫前期、子痫或HELLP综合征的女性中,255例(35.4%)在分娩前接受了硫酸镁治疗。41%的病房报告尽可能对所有子痫前期患者使用硫酸镁,且使用硫酸镁的频率高于有时使用的病房。在无子痫前期的女性中,95例(2.6%)接受了硫酸镁治疗。9个病房(7.6%)报告尽可能使用硫酸镁进行胎儿神经保护。在这些病房中,无重度子痫前期、子痫和HELLP综合征分娩时硫酸镁的使用中位数为14.3%。只有1个病房报告将硫酸镁用作一线宫缩抑制剂。在无子痫前期的女性中,因早产临产而在分娩前住院的女性中硫酸镁的使用率并不更高。
重度子痫前期、子痫或HELLP综合征的治疗中,硫酸镁的使用频率未达到循证医学的推荐水平。硫酸镁很少用于胎儿神经保护,且不再用于抑制宫缩。为持续降低发病率,需要更加关注硫酸镁的使用。