Lee Yun Jeong, Yum Mi Sun, Kim Eun Hee, Kim Min Jee, Kim Kyung Mo, Im Ho Joon, Kim Young Hwue, Park Young Seo, Ko Tae Sung
Department of Pediatrics, Kyungpook National University Hospital, Daegu, Korea.
Department of Pediatrics, Asan Medical Center Children's Hospital, University of Ulsan College of Medicine, Seoul, Korea.
J Korean Med Sci. 2017 Mar;32(3):457-464. doi: 10.3346/jkms.2017.32.3.457.
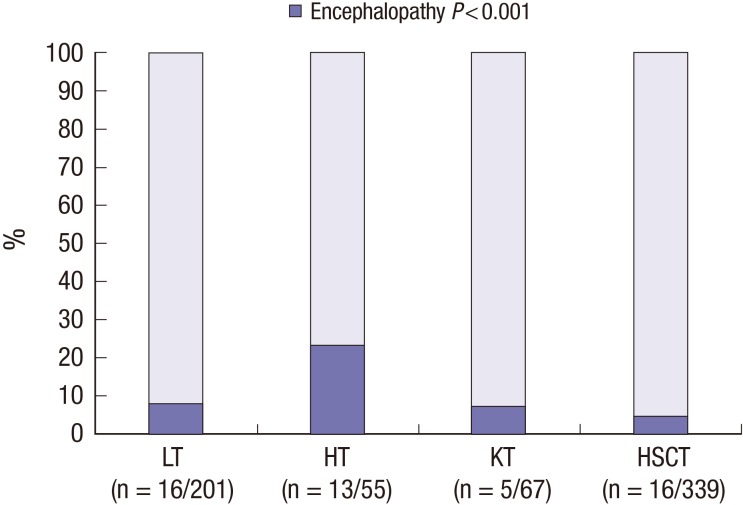
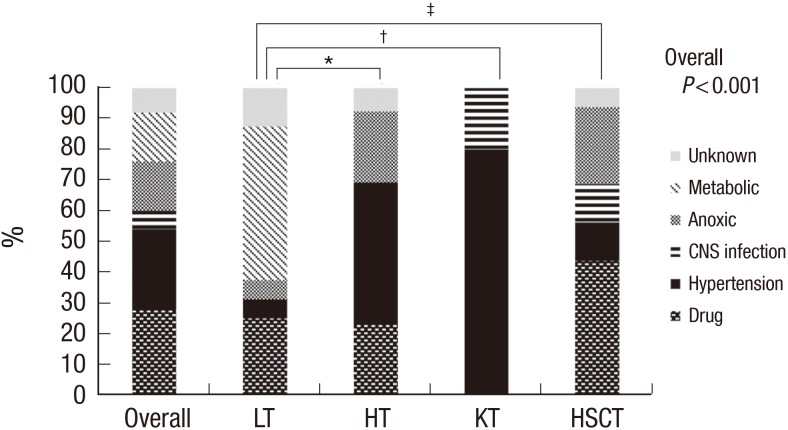
We aimed to analyze characteristics of encephalopathy after both hematopoietic stem cell and solid organ pediatric transplantation. We retrospectively reviewed medical records of 662 pediatric transplant recipients (201 with liver transplantation [LT], 55 with heart transplantation [HT], and 67 with kidney transplantation [KT], 339 with allogeneic hematopoietic stem cell transplantation [HSCT]) who received their graft organs at Asan Medical Center between January 2000 and July 2014. Of the 662 patients, 50 (7.6%) experienced encephalopathy after transplantation. The incidence of encephalopathy was significantly different according to the type of organ transplant: LT, 16/201 (8.0%), HT, 13/55 (23.6%), KT, 5/67 (7.5%), and HSCT, 16/339 (4.7%) (P < 0.001). Drug-induced encephalopathy (n = 14) was the most common encephalopathy for all transplant types, but particularly after HSCT. Hypertensive encephalopathy was the most common after KT and HT, whereas metabolic encephalopathy was the most common after LT. The median time to encephalopathy onset also differed according to the transplant type: 5 days after KT (range 0-491 days), 10 days after HT (1-296 days), 49.5 days after HSCT (9-1,405 days), and 39 days after LT (1-1,092 days) (P = 0.018). The mortality rate among patients with encephalopathy was 42.0% (n = 21/50). Only 5 patients died of neurologic complications. Transplant-associated encephalopathy presented different characteristics according to the type of transplant. Specialized diagnostic approach for neurologic complications specific to the type of transplant may improve survival and quality of life in children after transplantation.
我们旨在分析小儿造血干细胞移植和实体器官移植后脑病的特征。我们回顾性分析了2000年1月至2014年7月在峨山医学中心接受移植器官的662例小儿移植受者的医疗记录(201例肝移植[LT],55例心脏移植[HT],67例肾移植[KT],339例异基因造血干细胞移植[HSCT])。在这662例患者中,50例(7.6%)在移植后出现脑病。根据器官移植类型,脑病的发生率有显著差异:LT为16/201(8.0%),HT为13/55(23.6%),KT为5/67(7.5%),HSCT为16/339(4.7%)(P<0.001)。药物性脑病(n = 14)是所有移植类型中最常见的脑病,尤其是在HSCT后。高血压脑病在KT和HT后最常见,而代谢性脑病在LT后最常见。脑病发病的中位时间也因移植类型而异:KT后5天(范围0 - 491天),HT后10天(1 - 296天),HSCT后49.5天(9 - 1405天),LT后39天(1 - 1092天)(P = 0.018)。脑病患者的死亡率为42.0%(n = 21/50)。只有5例死于神经系统并发症。移植相关脑病根据移植类型呈现不同特征。针对特定移植类型的神经系统并发症的专业诊断方法可能会提高小儿移植后的生存率和生活质量。