Department of Critical Care Medicine, Nanjing ZhongDa Hospital, School of Medicine, Southeast University, 87 Dingjiaqiao Road, Gulou District, Nanjing, Jiangsu, 210009, China.
Crit Care. 2017 Feb 3;21(1):23. doi: 10.1186/s13054-017-1600-x.
The effect of alterations in tidal volume on mortality of acute respiratory distress syndrome (ARDS) is determined by respiratory system compliance. We aimed to investigate the effects of different tidal volumes on lung strain in ARDS patients who had various levels of respiratory system compliance.
Nineteen patients were divided into high (C group) and low (C group) respiratory system compliance groups based on their respiratory system compliance values. We defined compliance ≥0.6 ml/(cmHO/kg) as C and compliance <0.6 ml/(cmHO/kg) as C. End-expiratory lung volumes (EELV) at various tidal volumes were measured by nitrogen wash-in/washout. Lung strain was calculated as the ratio between tidal volume and EELV. The primary outcome was that lung strain is a function of tidal volume in patients with various levels of respiratory system compliance.
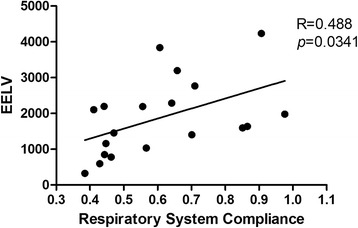
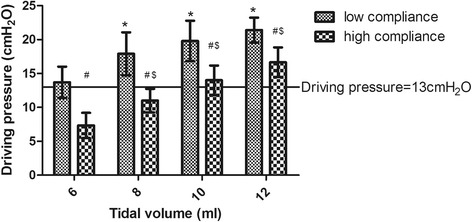
The mean baseline EELV, strain and respiratory system compliance values were 1873 ml, 0.31 and 0.65 ml/(cmHO/kg), respectively; differences in all of these parameters were statistically significant between the two groups. For all participants, a positive correlation was found between the respiratory system compliance and EELV (R = 0.488, p = 0.034). Driving pressure and strain increased together as the tidal volume increased from 6 ml/kg predicted body weight (PBW) to 12 ml/kg PBW. Compared to the C ARDS patients, the driving pressure was significantly higher in the C patients at each tidal volume. Similar effects of lung strain were found for tidal volumes of 6 and 8 ml/kg PBW. The "lung injury" limits for driving pressure and lung strain were much easier to exceed with increases in the tidal volume in C patients.
Respiratory system compliance affected the relationships between tidal volume and driving pressure and lung strain in ARDS patients. These results showed that increasing tidal volume induced lung injury more easily in patients with low respiratory system compliance.
Clinicaltrials.gov identifier NCT01864668 , Registered 21 May 2013.
潮气量变化对急性呼吸窘迫综合征(ARDS)死亡率的影响取决于呼吸系统顺应性。我们旨在研究不同潮气量对呼吸系统顺应性不同的 ARDS 患者肺应变的影响。
19 名患者根据呼吸系统顺应性值分为高(C 组)和低(C 组)呼吸系统顺应性组。我们将顺应性≥0.6ml/(cmHO/kg)定义为 C,顺应性<0.6ml/(cmHO/kg)定义为 C。通过氮气吸入/呼出法测量不同潮气量下的呼气末肺容量(EELV)。肺应变计算为潮气量与 EELV 的比值。主要结局是肺应变是呼吸系统顺应性不同的患者的潮气量的函数。
两组患者的平均基线 EELV、应变和呼吸系统顺应性值分别为 1873ml、0.31 和 0.65ml/(cmHO/kg),两组间所有参数均存在统计学差异。所有参与者的呼吸系统顺应性与 EELV 呈正相关(R=0.488,p=0.034)。随着潮气量从 6ml/kg 预测体重(PBW)增加到 12ml/kg PBW,驱动压力和应变一起增加。与 C ARDS 患者相比,在每个潮气量下,C 患者的驱动压力均显著升高。在 6ml/kg 和 8ml/kg PBW 潮气量下,也发现了相似的肺应变效应。在 C 患者中,随着潮气量的增加,驱动压力和肺应变的“肺损伤”限值更容易超过。
呼吸系统顺应性影响 ARDS 患者潮气量与驱动压力和肺应变之间的关系。这些结果表明,在呼吸系统顺应性较低的患者中,增加潮气量更容易引起肺损伤。
Clinicaltrials.gov 标识符 NCT01864668,于 2013 年 5 月 21 日注册。