Onodera Yu, Nakano Toru, Heishi Takahiro, Sakurai Tadashi, Taniyama Yusuke, Sato Chiaki, Ohuchi Noriaki, Kamei Takashi
Division of Advanced Surgical Science and Technology, Tohoku University Graduate School of Medicine, Sendai, Miyagi, 980-8574, Japan.
Division of Advanced Surgical Science and Technology, Tohoku University Graduate School of Medicine, Sendai, Miyagi, 980-8574, Japan.
Int J Surg Case Rep. 2017;31:154-158. doi: 10.1016/j.ijscr.2017.01.040. Epub 2017 Jan 19.
The incidence of lymph node metastasis in the dorsal area of the thoracic aorta (DTA) is relatively low in patients with esophageal cancer. It is difficult to approach the DTA using surgical procedures, such as an open thoracotomy and thoracoscopy in the left decubitus position.
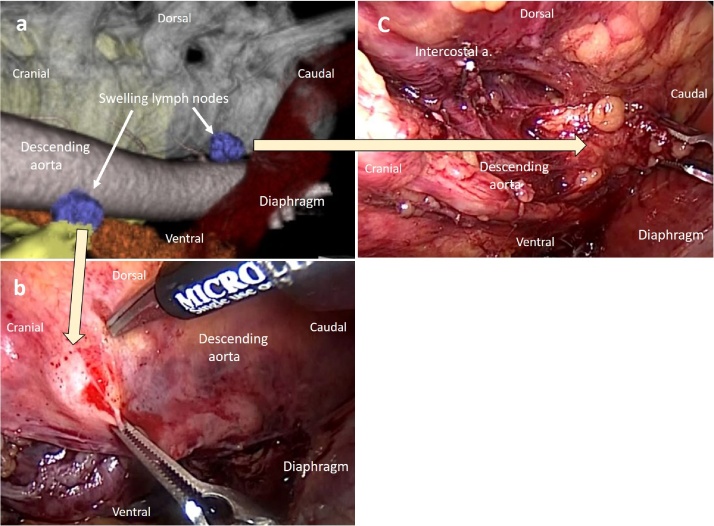
Case 1: A 70-year-old man with esophageal cancer underwent thoracoscopic esophagectomy with mediastinal lymph node dissection via a right thoracoscopic approach, followed by lymphadenectomy in the DTA via left thoracoscopy in the prone position. Microscopic findings revealed two metastatic lymph nodes in the DTA. The definitive diagnosis was squamous cell carcinoma of the esophagus, and the pathological stage was T2N3M0 (Union for International Cancer Control [UICC], 7th edition). The patient showed lung metastasis 8 months after the surgery. Case 2: A 72-year-old man with esophageal cancer underwent esophagectomy via a bilateral approach in the prone position, using a similar procedure as in case 1. The definitive diagnosis was squamous cell carcinoma of the esophagus, and the pathological stage was T3N2M0. The patient showed a metastatic mediastinal lymph node 4 months after the surgery.
Bilateral thoracoscopic esophagectomy in the prone position can be safely performed, and it might be an alternative curative surgery for esophageal cancer. However, both our cases showed metastasis in the early postoperative period. The long-term outcome and significance of dissection of lymph nodes in the DTA in patients with esophageal cancer remains controversial. Further studies are required to establish the indications and efficacy of this therapeutic approach.
食管癌患者胸主动脉背侧区域(DTA)的淋巴结转移发生率相对较低。采用诸如开胸手术和左侧卧位胸腔镜检查等外科手术方法难以触及DTA。
病例1:一名70岁食管癌男性患者接受了经右胸腹腔镜入路的胸腔镜食管切除术及纵隔淋巴结清扫术,随后在俯卧位经左胸腹腔镜进行DTA淋巴结切除术。显微镜检查发现DTA有两个转移淋巴结。最终诊断为食管鳞状细胞癌,病理分期为T2N3M0(国际癌症控制联盟[UICC]第7版)。患者术后8个月出现肺转移。病例2:一名72岁食管癌男性患者采用与病例1类似的手术方法,在俯卧位经双侧入路进行食管切除术。最终诊断为食管鳞状细胞癌,病理分期为T3N2M0。患者术后4个月出现纵隔淋巴结转移。
俯卧位双侧胸腔镜食管切除术可安全实施,可能是食管癌的一种替代根治性手术。然而,我们的两个病例均在术后早期出现转移。食管癌患者DTA淋巴结清扫的长期疗效及意义仍存在争议。需要进一步研究以确定这种治疗方法的适应证和疗效。