Jiang Hong, Qian Xu, Carroli Guillermo, Garner Paul
Department of Maternal, Child and Adolescent Health, School of Public Health, Fudan University, Mailbox 175, No. 138 Yi Xue Yuan Road, Shanghai, Shanghai, China, 200032.
Centro Rosarino de Estudios Perinatales (CREP), Moreno 878 piso 6, Rosario, Santa Fe, Argentina, 2000.
Cochrane Database Syst Rev. 2017 Feb 8;2(2):CD000081. doi: 10.1002/14651858.CD000081.pub3.
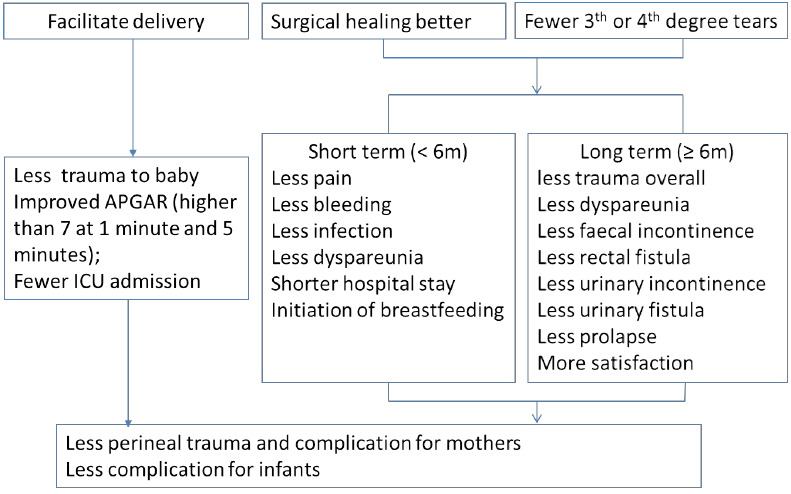
Some clinicians believe that routine episiotomy, a surgical cut of the vagina and perineum, will prevent serious tears during childbirth. On the other hand, an episiotomy guarantees perineal trauma and sutures.
To assess the effects on mother and baby of a policy of selective episiotomy ('only if needed') compared with a policy of routine episiotomy ('part of routine management') for vaginal births.
We searched Cochrane Pregnancy and Childbirth's Trials Register (14 September 2016) and reference lists of retrieved studies.
Randomised controlled trials (RCTs) comparing selective versus routine use of episiotomy, irrespective of parity, setting or surgical type of episiotomy. We included trials where either unassisted or assisted vaginal births were intended. Quasi-RCTs, trials using a cross-over design or those published in abstract form only were not eligible for inclusion in this review.
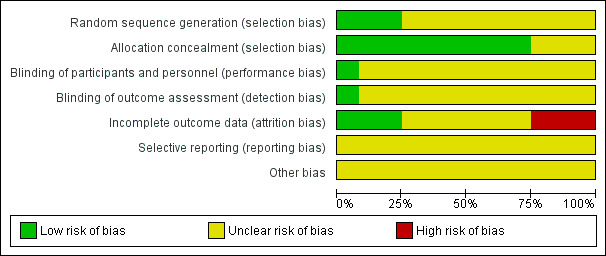
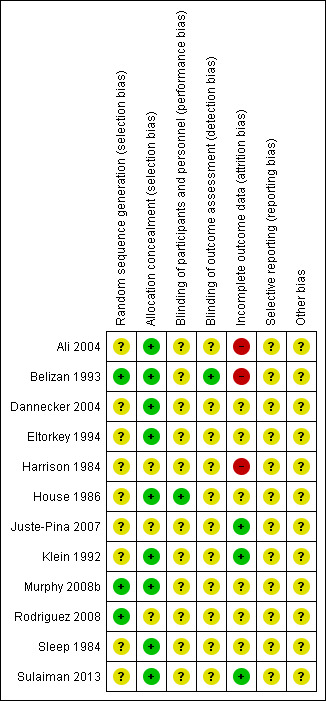
Two authors independently screened studies, extracted data, and assessed risk of bias. A third author mediated where there was no clear consensus. We observed good practice for data analysis and interpretation where trialists were review authors. We used fixed-effect models unless heterogeneity precluded this, expressed results as risk ratios (RR) and 95% confidence intervals (CI), and assessed the certainty of the evidence using GRADE.
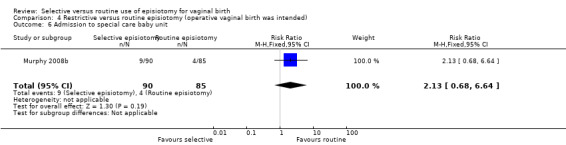
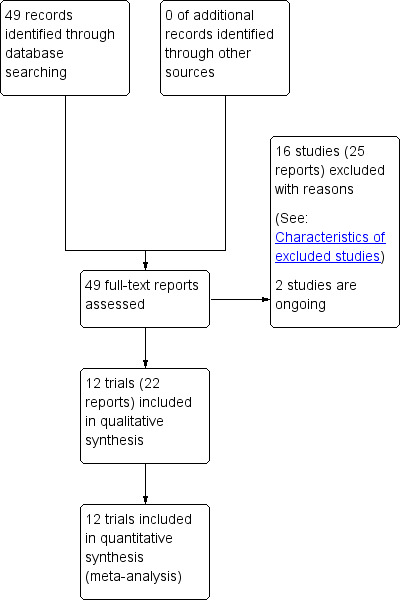
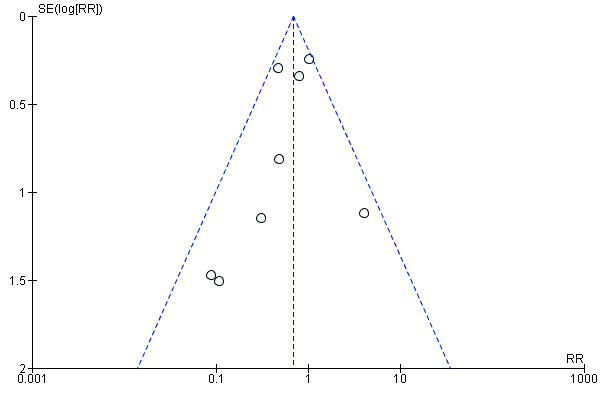
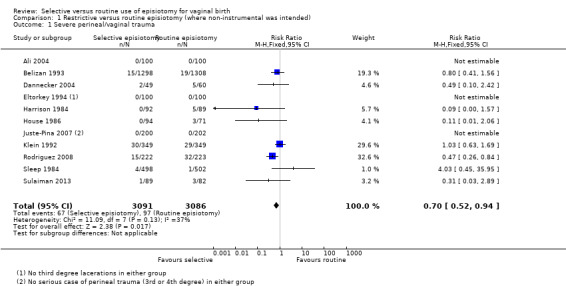
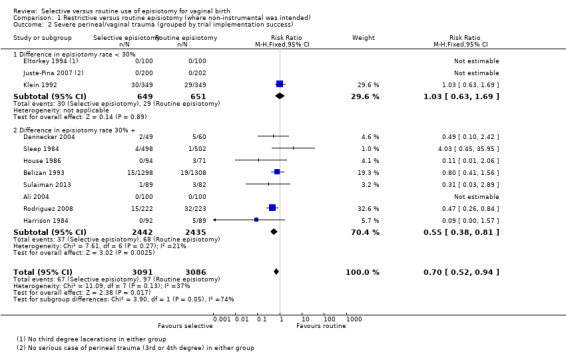
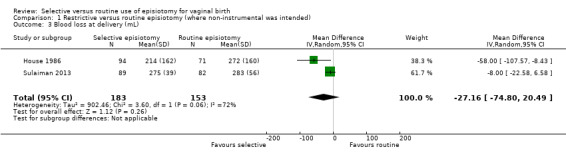
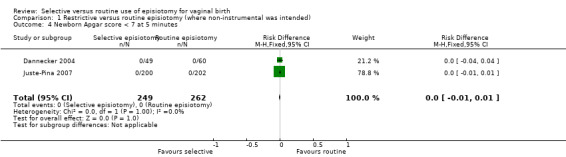
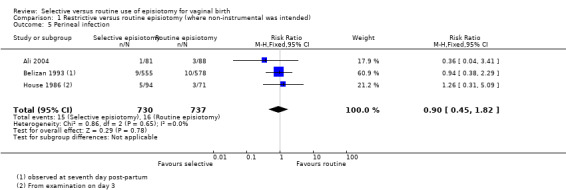
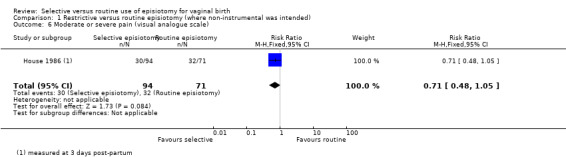
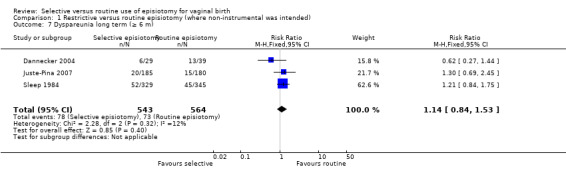
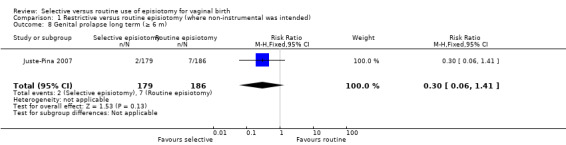
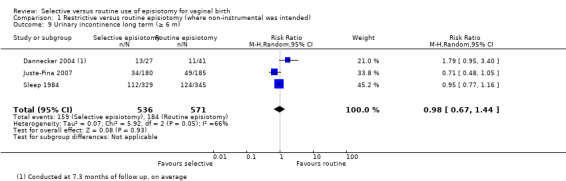
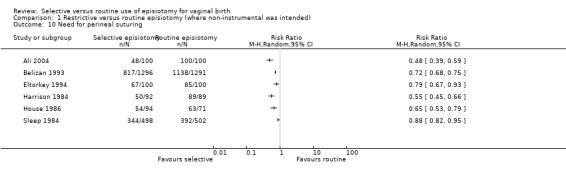
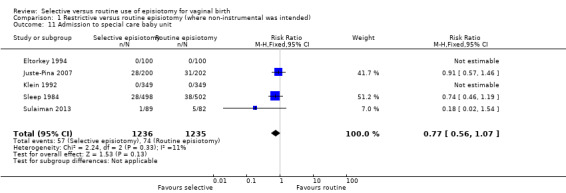
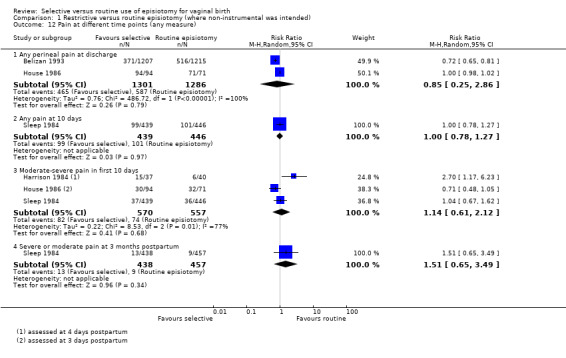
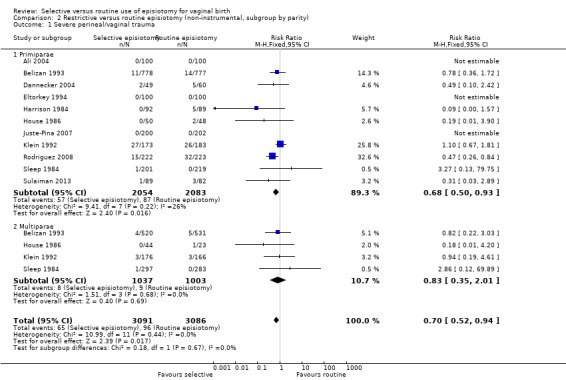
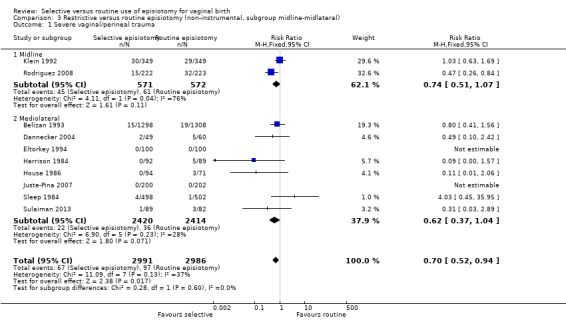
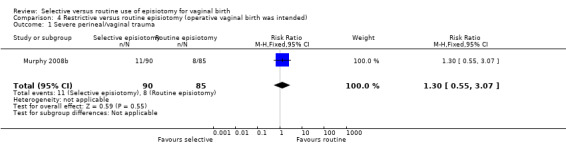
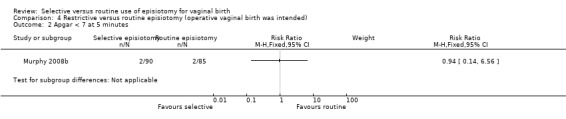
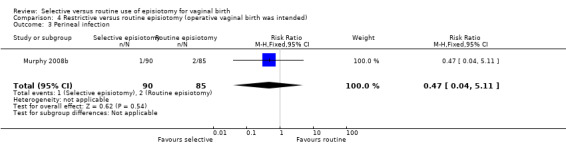
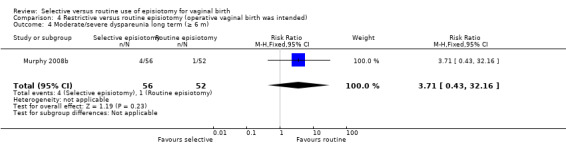
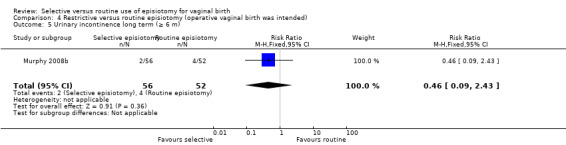
This updated review includes 12 studies (6177 women), 11 in women in labour for whom a vaginal birth was intended, and one in women where an assisted birth was anticipated. Two were trials each with more than 1000 women (Argentina and the UK), and the rest were smaller (from Canada, Germany, Spain, Ireland, Malaysia, Pakistan, Columbia and Saudi Arabia). Eight trials included primiparous women only, and four trials were in both primiparous and multiparous women. For risk of bias, allocation was adequately concealed and reported in nine trials; sequence generation random and adequately reported in three trials; blinding of outcomes adequate and reported in one trial, blinding of participants and personnel reported in one trial.For women where an unassisted vaginal birth was anticipated, a policy of selective episiotomy may result in 30% fewer women experiencing severe perineal/vaginal trauma (RR 0.70, 95% CI 0.52 to 0.94; 5375 women; eight RCTs; low-certainty evidence). We do not know if there is a difference for blood loss at delivery (an average of 27 mL less with selective episiotomy, 95% CI from 75 mL less to 20 mL more; two trials, 336 women, very low-certainty evidence). Both selective and routine episiotomy have little or no effect on infants with Apgar score less than seven at five minutes (four trials, no events; 3908 women, moderate-certainty evidence); and there may be little or no difference in perineal infection (RR 0.90, 95% CI 0.45 to 1.82, three trials, 1467 participants, low-certainty evidence).For pain, we do not know if selective episiotomy compared with routine results in fewer women with moderate or severe perineal pain (measured on a visual analogue scale) at three days postpartum (RR 0.71, 95% CI 0.48 to 1.05, one trial, 165 participants, very low-certainty evidence). There is probably little or no difference for long-term (six months or more) dyspareunia (RR1.14, 95% CI 0.84 to 1.53, three trials, 1107 participants, moderate-certainty evidence); and there may be little or no difference for long-term (six months or more) urinary incontinence (average RR 0.98, 95% CI 0.67 to 1.44, three trials, 1107 participants, low-certainty evidence). One trial reported genital prolapse at three years postpartum. There was no clear difference between the two groups (RR 0.30, 95% CI 0.06 to 1.41; 365 women; one trial, low certainty evidence). Other outcomes relating to long-term effects were not reported (urinary fistula, rectal fistula, and faecal incontinence). Subgroup analyses by parity (primiparae versus multiparae) and by surgical method (midline versus mediolateral episiotomy) did not identify any modifying effects. Pain was not well assessed, and women's preferences were not reported.One trial examined selective episiotomy compared with routine episiotomy in women where an operative vaginal delivery was intended in 175 women, and did not show clear difference on severe perineal trauma between the restrictive and routine use of episiotomy, but the analysis was underpowered.
AUTHORS' CONCLUSIONS: In women where no instrumental delivery is intended, selective episiotomy policies result in fewer women with severe perineal/vaginal trauma. Other findings, both in the short or long term, provide no clear evidence that selective episiotomy policies results in harm to mother or baby.The review thus demonstrates that believing that routine episiotomy reduces perineal/vaginal trauma is not justified by current evidence. Further research in women where instrumental delivery is intended may help clarify if routine episiotomy is useful in this particular group. These trials should use better, standardised outcome assessment methods.
一些临床医生认为,常规会阴切开术(一种对阴道和会阴的外科切割)可预防分娩时的严重撕裂伤。另一方面,会阴切开术会导致会阴创伤和缝合。
评估选择性会阴切开术(“仅在必要时”)与常规会阴切开术(“常规处理的一部分”)策略对阴道分娩母婴的影响。
我们检索了Cochrane妊娠与分娩试验注册库(2016年9月14日)以及检索到的研究的参考文献列表。
比较选择性与常规使用会阴切开术的随机对照试验(RCT),不考虑产次、分娩环境或会阴切开术的手术类型。我们纳入了旨在进行非助产或助产阴道分娩的试验。准RCT、采用交叉设计的试验或仅以摘要形式发表的试验均不符合本综述的纳入标准。
两位作者独立筛选研究、提取数据并评估偏倚风险。在没有明确共识的情况下,由第三位作者进行协调。当试验者为综述作者时,我们观察到了良好的数据分析和解释方法。除非存在异质性,否则我们使用固定效应模型,将结果表示为风险比(RR)和95%置信区间(CI),并使用GRADE评估证据的确定性。
本更新综述纳入了12项研究(6177名女性),其中11项针对计划进行阴道分娩的分娩期女性,1项针对预计进行助产分娩的女性。两项试验每项涉及超过1000名女性(阿根廷和英国),其余试验规模较小(来自加拿大、德国、西班牙、爱尔兰、马来西亚、巴基斯坦、哥伦比亚和沙特阿拉伯)。八项试验仅纳入初产妇,四项试验纳入了初产妇和经产妇。关于偏倚风险,九项试验中分配方案得到了充分隐藏和报告;三项试验中随机序列生成随机且报告充分;一项试验中结局盲法充分且报告充分,一项试验中参与者和人员盲法得到报告。对于预计进行非助产阴道分娩的女性,选择性会阴切开术策略可能会使经历严重会阴/阴道创伤的女性减少30%(RR 0.70,95%CI 0.52至0.94;5375名女性;八项RCT;低确定性证据)。我们不知道分娩时失血是否存在差异(选择性会阴切开术平均少27 mL,95%CI从少75 mL至多20 mL;两项试验,336名女性;极低确定性证据)。选择性和常规会阴切开术对5分钟时阿氏评分低于7分的婴儿几乎没有影响(四项试验,无事件发生;3908名女性;中等确定性证据);会阴感染可能几乎没有差异(RR 0.90,95%CI 从0.45至1.82;三项试验,1467名参与者;低确定性证据)。对于疼痛,我们不知道与常规会阴切开术相比,选择性会阴切开术是否会使产后三天出现中度或重度会阴疼痛(采用视觉模拟评分法测量)的女性更少(RR 0.71,95%CI 0.48至1.05;一项试验,165名参与者;极低确定性证据)。长期(六个月或更长时间)性交困难可能几乎没有差异(RR 1.14,95%CI 0.84至1.53;三项试验,1107名参与者;中等确定性证据);长期(六个月或更长时间)尿失禁可能几乎没有差异(平均RR 0.98,95%CI 0.67至1.44;三项试验,1107名参与者;低确定性证据)。一项试验报告了产后三年的生殖器脱垂情况。两组之间没有明显差异(RR 0.30,95%CI 0.06至1.41;365名女性;一项试验;低确定性证据)。未报告其他与长期影响相关的结局(尿瘘、直肠瘘和大便失禁)。按产次(初产妇与经产妇)和手术方法(中线会阴切开术与侧斜会阴切开术)进行的亚组分析未发现任何修饰效应。疼痛评估不佳,且未报告女性的偏好。一项试验在175名计划进行手术阴道分娩女性中比较了选择性会阴切开术与常规会阴切开术,在会阴切开术的限制性使用和常规使用之间,严重会阴创伤方面未显示出明显差异,但分析的效力不足。
对于不打算进行器械助产的女性,选择性会阴切开术策略可减少严重会阴/阴道创伤的女性数量。短期或长期的其他研究结果均未提供明确证据表明选择性会阴切开术策略会对母婴造成伤害。因此,本综述表明,目前的证据并不支持认为常规会阴切开术可减少会阴/阴道创伤的观点。对计划进行器械助产的女性进行进一步研究,可能有助于明确常规会阴切开术在这一特定群体中是否有用。这些试验应采用更好的、标准化的结局评估方法。