Bae Sun Hyun, Kim Dong Wook, Kim Mi-Sook, Shin Myung-Hee, Park Hee Chul, Lim Do Hoon
Department of Radiation Oncology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Radiat Oncol J. 2017 Mar;35(1):78-89. doi: 10.3857/roj.2016.01942. Epub 2017 Feb 13.
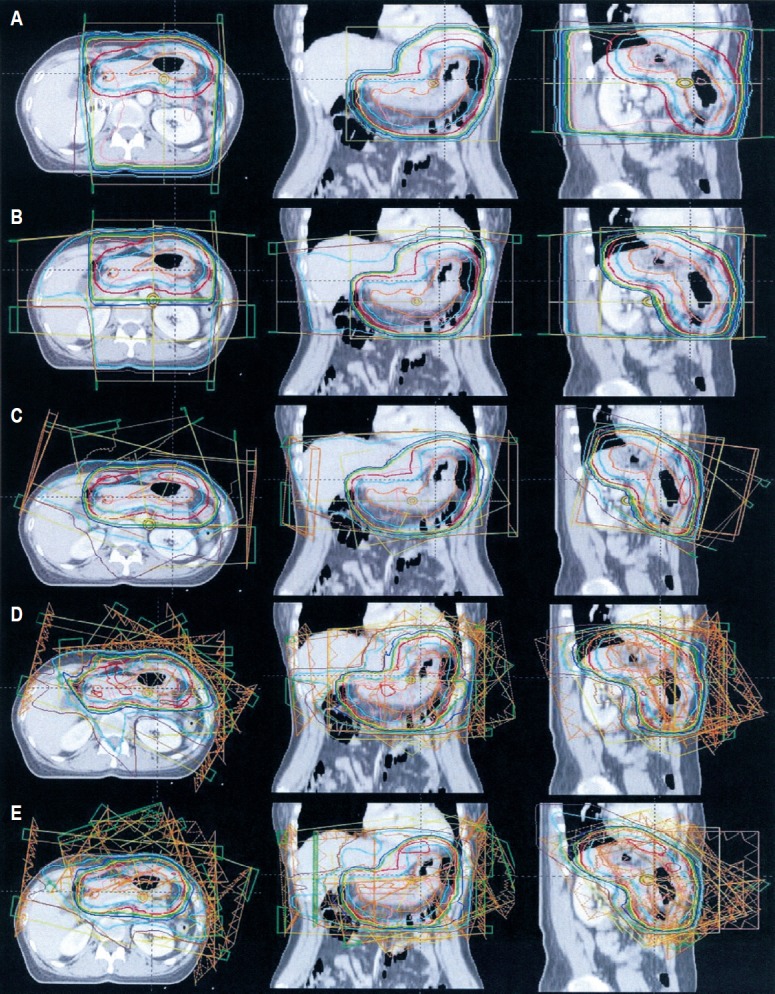
To determine the optimal radiotherapy technique for gastric mucosa-associated lymphoid tissue lymphoma (MALToma), we compared the dosimetric parameters and the risk of solid secondary cancer from scattered doses among anterior-posterior/posterior-anterior parallel-opposed fields (AP/PA), anterior, posterior, right, and left lateral fields (4_field), 3-dimensional conformal radiotherapy (3D-CRT) using noncoplanar beams, and intensity-modulated radiotherapy composed of 7 coplanar beams (IMRT_co) and 7 coplanar and noncoplanar beams (IMRT_non).
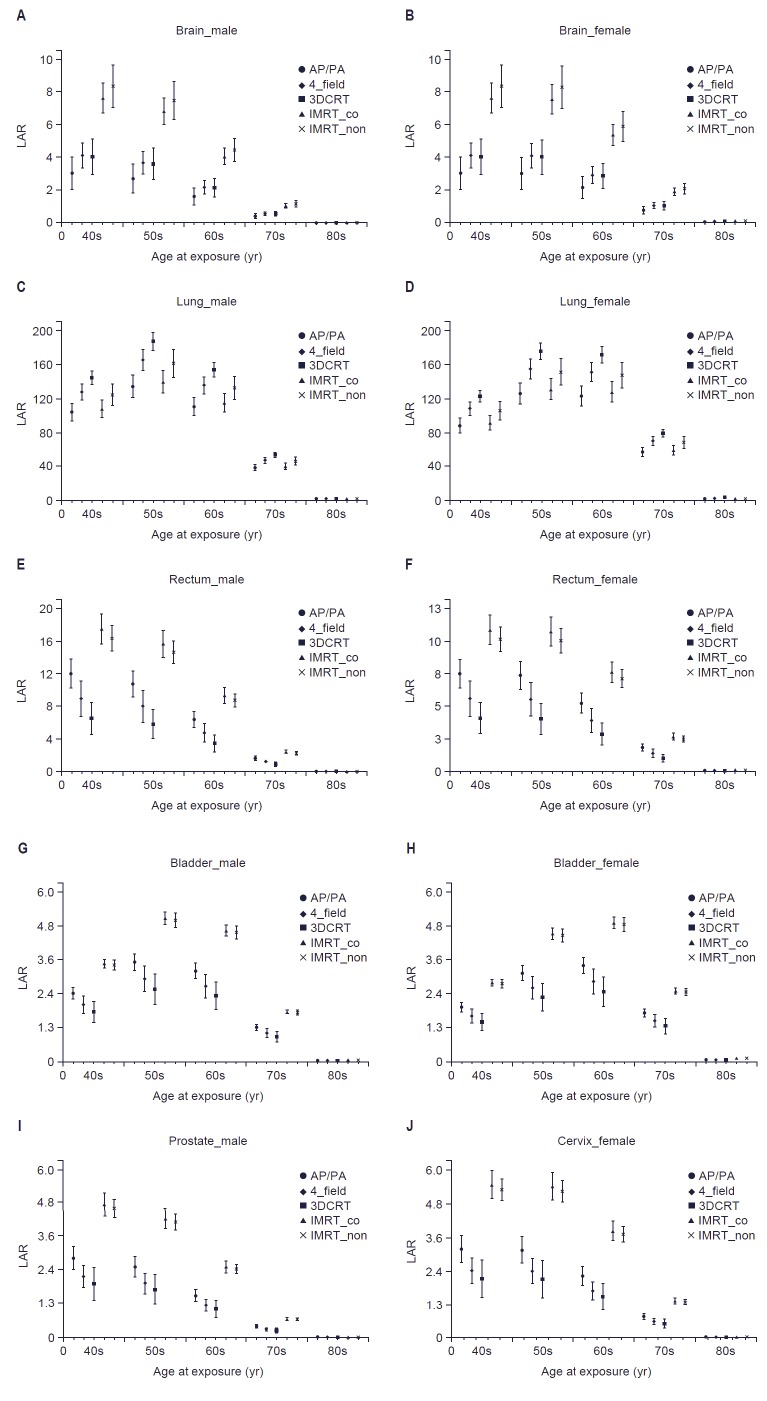
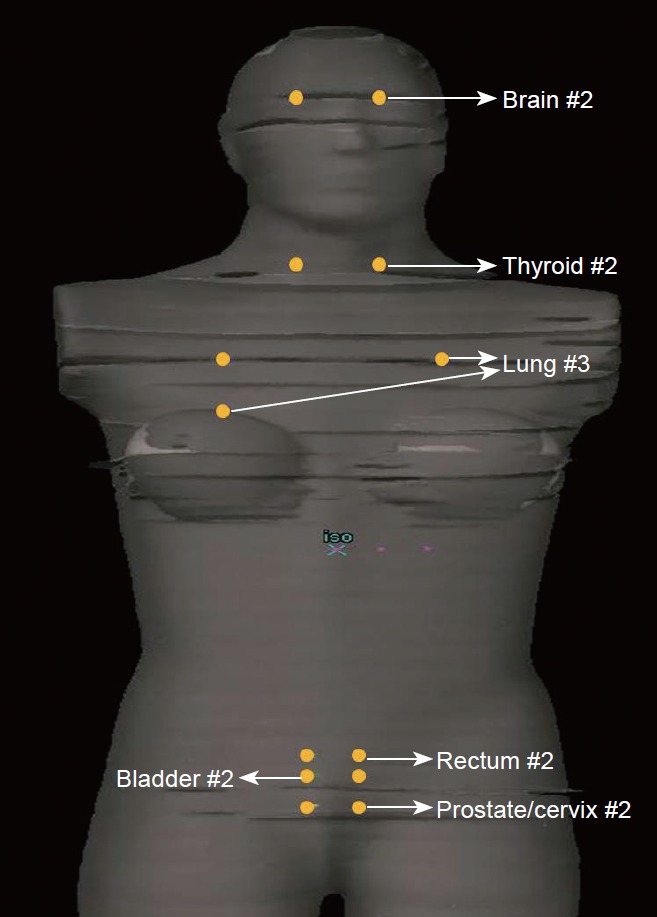
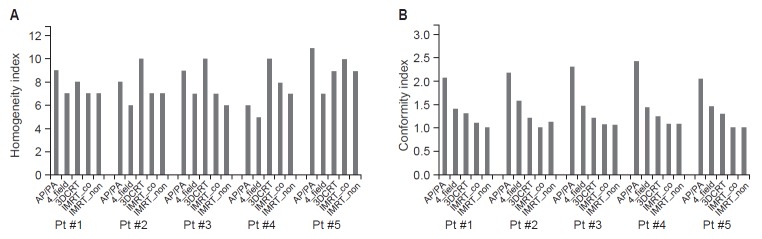
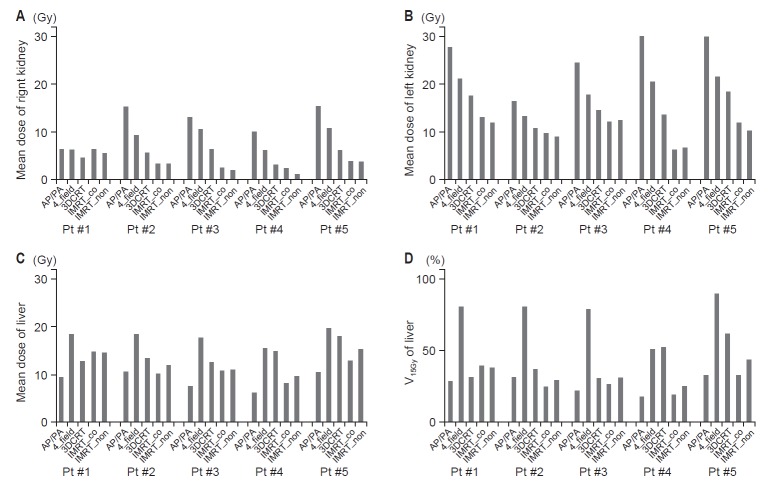
We retrospectively generated 5 planning techniques for 5 patients with gastric MALToma. Homogeneity index (HI), conformity index (CI), and mean doses of the kidney and liver were calculated from the dose-volume histograms. Applied the Biological Effects of Ionizing Radiation VII report to scattered doses, the lifetime attributable risk (LAR) was calculated to estimate the risk of solid secondary cancer.
The best value of CI was obtained with IMRT, although the HI varied among patients. The mean kidney dose was the highest with AP/PA, followed by 4_field, 3D-CRT, IMRT_co, and IMRT_non. On the other hand, the mean liver dose was the highest with 4_field and the lowest with AP/PA. Compared with 4_field, the LAR for 3D-CRT decreased except the lungs, and the LAR for IMRT_co and IMRT_non increased except the lungs. However, the absolute differences were much lower than <1%.
Tailored RT techniques seem to be beneficial because it could achieve adjacent organ sparing with very small and clinically irrelevant increase of secondary solid cancer risk compared to the conventional techniques.
为确定胃黏膜相关淋巴组织淋巴瘤(MALToma)的最佳放疗技术,我们比较了前后/后前对穿野(AP/PA)、前野、后野、右野和左野(4野)、使用非共面射束的三维适形放疗(3D-CRT)以及由7个共面射束组成的调强放疗(IMRT_co)和7个共面及非共面射束组成的调强放疗(IMRT_non)的剂量学参数以及散射线所致实体继发癌风险。
我们回顾性地为5例胃MALToma患者生成了5种放疗计划技术。从剂量体积直方图中计算均匀性指数(HI)、适形性指数(CI)以及肾脏和肝脏的平均剂量。将《电离辐射的生物学效应VII报告》应用于散射线剂量,计算终生归因风险(LAR)以估计实体继发癌风险。
IMRT获得了最佳的CI值,尽管HI在患者之间有所不同。AP/PA的平均肾脏剂量最高,其次是4野、3D-CRT、IMRT_co和IMRT_non。另一方面,4野的平均肝脏剂量最高,AP/PA的最低。与4野相比,3D-CRT除肺部外的LAR降低,IMRT_co和IMRT_non除肺部外的LAR升高。然而,绝对差异远低于<1%。
定制的放疗技术似乎是有益的,因为与传统技术相比,它可以在实体继发癌风险非常小且临床上无关紧要的增加的情况下实现对相邻器官的保护。