Nattabi Barbara, Matthews Veronica, Bailie Jodie, Rumbold Alice, Scrimgeour David, Schierhout Gill, Ward James, Guy Rebecca, Kaldor John, Thompson Sandra C, Bailie Ross
Western Australian Centre for Rural Health, University of Western Australia, 167 Fitzgerald Street, Geraldton, WA, 6530, Australia.
Menzies School of Health Research, Brisbane, QLD, Australia.
BMC Infect Dis. 2017 Feb 15;17(1):148. doi: 10.1186/s12879-017-2241-z.
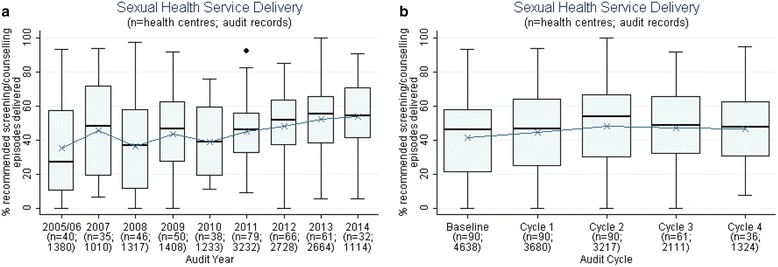
Chlamydia, gonorrhoea and syphilis are readily treatable sexually transmitted infections (STIs) which continue to occur at high rates in Australia, particularly among Aboriginal Australians. This study aimed to: explore the extent of variation in delivery of recommended STI screening investigations and counselling within Aboriginal primary health care (PHC) centres; identify the factors associated with variation in screening practices; and determine if provision of STI testing and counselling increased with participation in continuous quality improvement (CQI).
Preventive health audits (n = 16,086) were conducted at 137 Aboriginal PHC centres participating in the Audit and Best Practice for Chronic Disease Program, 2005-2014. STI testing and counselling data were analysed to determine levels of variation in chlamydia, syphilis and gonorrhoea testing and sexual health discussions. Multilevel logistic regression was used to determine factors associated with higher levels of STI-related service delivery and to quantify variation attributable to health centre and client characteristics.
Significant variation in STI testing and counselling exists among Aboriginal PHC centres with health centre factors accounting for 43% of variation between health centres and jurisdictions. Health centre factors independently associated with higher levels of STI testing and counselling included provision of an adult health check (odds ratio (OR) 3.40; 95% Confidence Interval (CI) 3.07-3.77) and having conducted 1-2 cycles of CQI (OR 1.34; 95% CI 1.16-1.55). Client factors associated with higher levels of STI testing and counselling were being female (OR 1.45; 95% CI 1.33-1.57), Aboriginal (OR 1.46; 95% CI 1.15-1.84) and aged 20-24 years (OR 3.84; 95% CI 3.07-4.80). For females, having a Pap smear test was also associated with STI testing and counselling (OR 4.39; 95% CI 3.84-5.03). There was no clear association between CQI experience beyond two CQI cycles and higher levels of documented delivery of STI testing and counselling services.
A number of Aboriginal PHC centres are achieving high rates of STI testing and counselling, while a significant number are not. STI-related service delivery could be substantially improved through focussed efforts to support health centres with relatively lower documented evidence of adherence to best practice guidelines.
衣原体、淋病和梅毒是易于治疗的性传播感染(STIs),在澳大利亚仍有很高的发病率,尤其是在澳大利亚原住民中。本研究旨在:探讨原住民初级卫生保健(PHC)中心在提供推荐的性传播感染筛查检查和咨询方面的差异程度;确定与筛查实践差异相关的因素;并确定参与持续质量改进(CQI)是否会增加性传播感染检测和咨询的提供。
在2005 - 2014年参与慢性病项目审计与最佳实践的137个原住民初级卫生保健中心进行了预防性健康审计(n = 16,086)。对性传播感染检测和咨询数据进行分析,以确定衣原体、梅毒和淋病检测以及性健康讨论的差异水平。采用多水平逻辑回归来确定与更高水平的性传播感染相关服务提供相关的因素,并量化可归因于健康中心和客户特征的差异。
原住民初级卫生保健中心之间在性传播感染检测和咨询方面存在显著差异,健康中心因素占健康中心和管辖区之间差异的43%。与更高水平的性传播感染检测和咨询独立相关的健康中心因素包括提供成人健康检查(优势比(OR)3.40;95%置信区间(CI)3.07 - 3.77)以及进行了1 - 2个周期的持续质量改进(OR 1.34;95% CI 1.16 - 1.55)。与更高水平的性传播感染检测和咨询相关的客户因素包括女性(OR 1.45;95% CI 1.33 - 1.57)、原住民(OR 1.46;95% CI 1.15 - 1.84)以及年龄在20 - 24岁之间(OR 3.84;95% CI 3.07 - 4.80)。对于女性,进行巴氏涂片检查也与性传播感染检测和咨询相关(OR 4.39;95% CI 3.84 - 5.03)。超过两个持续质量改进周期的持续质量改进经验与记录在案的性传播感染检测和咨询服务提供的更高水平之间没有明确关联。
一些原住民初级卫生保健中心实现了较高的性传播感染检测和咨询率,而相当一部分中心则没有。通过集中努力支持那些遵循最佳实践指南的记录证据相对较少的健康中心,可以大幅改善与性传播感染相关的服务提供。