Pinto Francisco Guerra, Thaunat Mathieu, Daggett Matt, Kajetanek Charles, Marques Tiago, Guimares Tales, Quelard Bénédicte, Sonnery-Cottet Bertrand
Hospital José de Almeida, Cascais, Portugal.
Centre Orthopédique Santy, FIFA Medical Center of Excellence, Générale de Santé, Hôpital Privé Jean Mermoz, Lyon, France.
Orthop J Sports Med. 2017 Jan 27;5(1):2325967116684121. doi: 10.1177/2325967116684121. eCollection 2017 Jan.
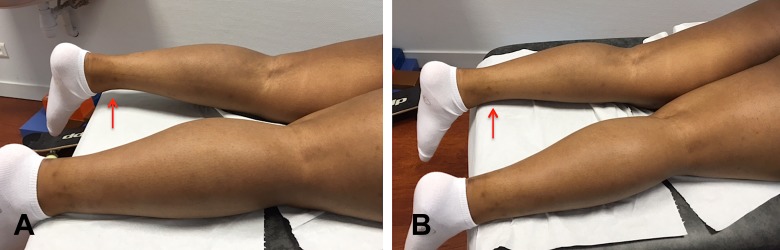
Cyclops syndrome is characterized by loss of terminal knee extension due to proliferative fibrous nodule formation in the intercondylar notch. This complication occurs in the early postoperative period after anterior cruciate ligament reconstruction (ACLR). The pathogenesis of Cyclops syndrome is not well understood.
Persistent hamstring contracture after ACLR is associated with an increased risk of subsequent Cyclops syndrome.
Case-control study; Level of evidence, 3.
The files of 45 patients who underwent arthroscopic debridement of a Cyclops lesion after ACLR were analyzed. Recorded data included demographic information and technical details of surgery. Preoperative magnetic resonance images were also analyzed, and patients with femoral bone bruising were identified. Passive and active range of motion were recorded in all patients preoperatively and at 3 and 6 weeks after surgery to address the Cyclops lesion. Passive extension deficit was evaluated in comparison with the contralateral limb and classified as secondary to hamstring contracture when contracture was observed and palpated in the prone position and when the extension deficit was reversed after exercises performed to fatigue the hamstrings. A control group was selected using a random numbers table among our entire ACLR cohort. Statistical analysis was performed to analyze differences between the 2 groups.
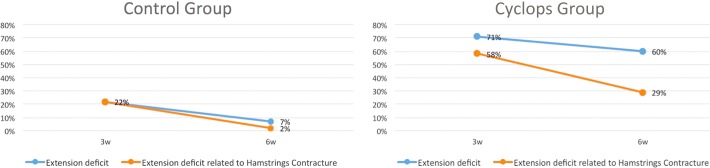
There was no significant difference between the groups with regard to age at ACLR, sex distribution, time from injury to surgery ( > .05), proportion of professional athletes, presence of femoral bone bruise, or technical aspects of surgery. The overall extension deficit incidence was significantly higher in the Cyclops group at 3 weeks (Cyclops, 71%; control, 22%) ( < .001) and at 6 weeks (Cyclops, 60%; control, 7%) ( < .001). The extension deficit related to hamstring contracture was significantly higher in the Cyclops group at 3 weeks (Cyclops, 58%; control, 22%) ( < .001) and at 6 weeks (Cyclops, 29%; control, 2%) ( < .001).
The Cyclops lesion is associated with a persistent hamstring contracture at 3 and 6 weeks after ACLR.
“独眼巨人综合征”的特征是由于髁间切迹处形成增殖性纤维结节导致膝关节终末伸展功能丧失。这种并发症发生在前交叉韧带重建(ACLR)术后早期。“独眼巨人综合征”的发病机制尚不完全清楚。
ACLR术后持续的腘绳肌挛缩与随后发生“独眼巨人综合征”的风险增加有关。
病例对照研究;证据等级,3级。
分析45例ACLR术后接受关节镜下“独眼巨人”病变清创术患者的病历。记录的数据包括人口统计学信息和手术技术细节。还分析了术前磁共振成像,并确定有股骨骨挫伤的患者。记录所有患者术前以及术后3周和6周针对“独眼巨人”病变时的被动和主动活动范围。与对侧肢体相比评估被动伸展不足情况,当在俯卧位观察到并触及挛缩且在进行使腘绳肌疲劳的运动后伸展不足情况得到改善时,将其归类为继发于腘绳肌挛缩。在整个ACLR队列中使用随机数字表选择一个对照组。进行统计分析以分析两组之间的差异。
两组在ACLR时的年龄、性别分布、受伤至手术的时间(P>.05)、职业运动员比例、股骨骨挫伤的存在情况或手术技术方面没有显著差异。“独眼巨人”组在术后3周(“独眼巨人”组,71%;对照组,22%)(P<.001)和6周(“独眼巨人”组,60%;对照组,7%)(P<.001)时总体伸展不足发生率显著更高。与腘绳肌挛缩相关的伸展不足在“独眼巨人”组术后3周(“独眼巨人”组,58%;对照组,22%)(P<.001)和6周(“独眼巨人”组,29%;对照组,2%)(P<.001)时显著更高。
“独眼巨人”病变与ACLR术后3周和6周时持续的腘绳肌挛缩有关。