Singh Gurshawn, Nassri Ammar, Kim David, Zhu Hong, Ramzan Zeeshan
Gurshawn Singh, Department of Medicine, Division of Gastroenterology and Hepatology, University of Texas Southwestern Medical Center at Dallas, Dallas, TX 75390, United States.
World J Gastrointest Pharmacol Ther. 2017 Feb 6;8(1):60-66. doi: 10.4292/wjgpt.v8.i1.60.
To determine if the lymphocyte-to-monocyte ratio (LMR) could be helpful in predicting survival in patients with pancreatic adenocarcinoma.
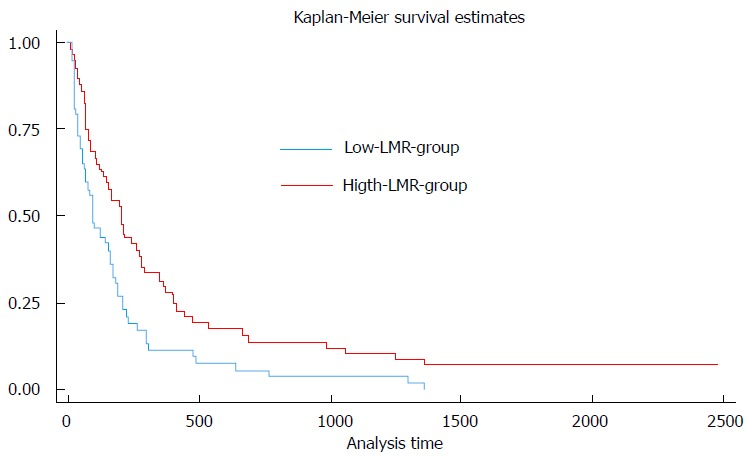
We retrospectively reviewed the medical records of all patients diagnosed with pancreatic adenocarcinoma in the VA North Texas Healthcare System from January 2005 to December 2010. The LMR was calculated from peripheral blood cell counts obtained at the time of diagnosis of pancreatic cancer by dividing the absolute lymphocyte count by the absolute monocyte count. A Univariable Cox regression analysis was performed using these data, and hazard ratios (HR) and 95%CI were calculated. The median LMR (2.05) was used to dichotomize patients into high-LMR and low-LMR groups and the log rank test was used to compare survival between the two groups.
We identified 97 patients with pancreatic adenocarcinoma (all men, 66% white, 30% African-American). The mean age and weight at diagnosis were 66.0 ± 0.9 (SEM) years and 80.4 ± 1.7 kg respectively. Mean absolute lymphocyte and monocyte values were 1.50 ± 0.07 K/μL and 0.74 ± 0.03 K/μL respectively. Mean, median and range of LMR was 2.36, 2.05 and 0.4-12 respectively. In the univariable Cox regression analysis, we found that an increased LMR was a significant indicator of improved overall survival in patients with pancreatic adenocarcinoma (HR = 0.83; 95%CI: 0.70-0.98; = 0.027). Kaplan-Meier analysis revealed an overall median survival of 128 d (95%CI: 80-162 d). The median survival of patients in the high-LMR (> 2.05) group was significantly greater than the low-LMR group (≤ 2.05) (194 d 93 d; = 0.03), validating a significant survival advantage in patients with a high LMR.
The LMR at diagnosis is a significant predictor for survival and can provide useful prognostic information in the management of patients with pancreatic adenocarcinoma.
确定淋巴细胞与单核细胞比值(LMR)是否有助于预测胰腺腺癌患者的生存期。
我们回顾性分析了2005年1月至2010年12月在弗吉尼亚州北德克萨斯医疗系统中所有被诊断为胰腺腺癌患者的病历。LMR通过将胰腺癌诊断时获得的外周血细胞计数中绝对淋巴细胞计数除以绝对单核细胞计数来计算。使用这些数据进行单变量Cox回归分析,并计算风险比(HR)和95%置信区间(CI)。中位LMR(2.05)用于将患者分为高LMR组和低LMR组,对数秩检验用于比较两组之间的生存期。
我们确定了97例胰腺腺癌患者(均为男性,66%为白人,30%为非裔美国人)。诊断时的平均年龄和体重分别为66.0±0.9(标准误)岁和80.4±1.7千克。平均绝对淋巴细胞和单核细胞值分别为1.50±0.07千/微升和0.74±0.03千/微升。LMR的平均值、中位数和范围分别为2.36、2.05和0.4 - 12。在单变量Cox回归分析中,我们发现LMR升高是胰腺腺癌患者总体生存期改善的显著指标(HR = 0.83;95%CI:0.70 - 0.98;P = 0.027)。Kaplan - Meier分析显示总体中位生存期为128天(95%CI:80 - 162天)。高LMR(> 2.05)组患者的中位生存期显著长于低LMR组(≤ 2.05)(194天对93天;P = 0.03),证实了高LMR患者具有显著的生存优势。
诊断时的LMR是生存期的显著预测指标,可为胰腺腺癌患者的管理提供有用的预后信息。