Zheng Zhiyuan, Han Xuesong, Guy Gery P, Davidoff Amy J, Li Chunyu, Banegas Matthew P, Ekwueme Donatus U, Yabroff K Robin, Jemal Ahmedin
Surveillance and Health Services Research Program, American Cancer Society, Atlanta, Georgia.
University of Maryland School of Pharmacy, Baltimore, Maryland.
Cancer. 2017 Apr 15;123(8):1453-1463. doi: 10.1002/cncr.30560. Epub 2017 Feb 20.
There is limited evidence from nationally representative samples about changes in prescription drug use for financial reasons among cancer survivors in the United States.
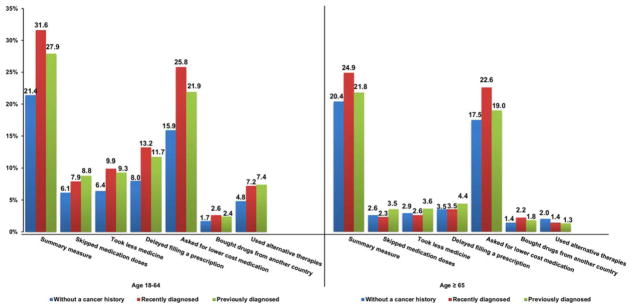
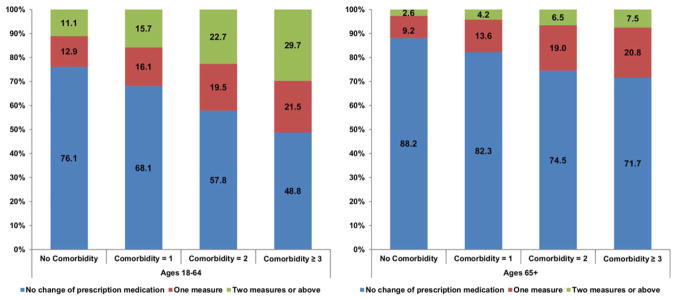
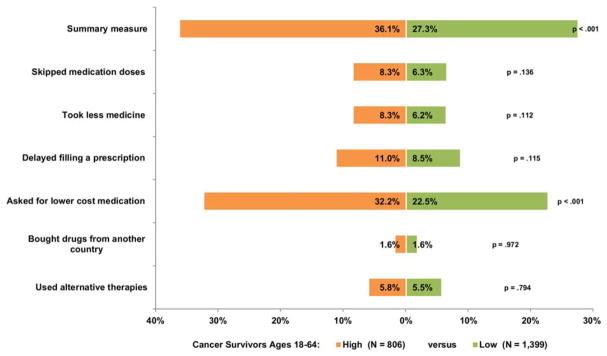
The 2011 to 2014 National Health Interview Survey was used to identify adults who reported ever having been told they had cancer (cancer survivors; n = 8931) and individuals without a cancer history (n = 126,287). Measures of changes in prescription drug use for financial reasons included: 1) skipping medication doses, 2) taking less medicine, 3) delaying filling a prescription, 4) asking a doctor for lower cost medication, 5) buying prescription drugs from another country, and 6) using alternative therapies. Multivariable logistic regression analyses were controlled for demographic characteristics, number of comorbid conditions, interactions between cancer history and number of comorbid conditions, and health insurance coverage. Main analyses were stratified by age (nonelderly, ages 18-64 years; elderly, ages ≥65 years) and time since diagnosis (recently diagnosed, <2 years; previously diagnosed, ≥2 years).
Among nonelderly individuals, both recently diagnosed (31.6%) and previously diagnosed (27.9%) cancer survivors were more likely to report any change in prescription drug use for financial reasons than those without a cancer history (21.4%), with the excess percentage changes for individual measures ranging from 3.5% to 9.9% among previously diagnosed survivors and from 2.6% to 2.7% among recently diagnosed survivors (P < .01). Elderly cancer survivors and those without a cancer history had comparable rates of changes in prescription drug use for financial reasons.
Nonelderly cancer survivors are particularly vulnerable to changes in prescription drug use for financial reasons, suggesting that targeted efforts are needed. Cancer 2017;123:1453-1463. © 2016 American Cancer Society.
在美国,关于癌症幸存者因经济原因导致处方药使用变化的全国代表性样本证据有限。
利用2011年至2014年的全国健康访谈调查,确定报告曾被告知患有癌症的成年人(癌症幸存者;n = 8931)和无癌症病史的个体(n = 126,287)。因经济原因导致处方药使用变化的衡量指标包括:1)漏服药物剂量,2)减少用药量,3)延迟配药,4)要求医生开低成本药物,5)从其他国家购买处方药,6)使用替代疗法。多变量逻辑回归分析对人口统计学特征、合并症数量、癌症病史与合并症数量之间的相互作用以及医疗保险覆盖情况进行了控制。主要分析按年龄(非老年人,18 - 64岁;老年人,≥65岁)和确诊后的时间(近期确诊,<2年;既往确诊,≥2年)进行分层。
在非老年人中,近期确诊的癌症幸存者(31.6%)和既往确诊的癌症幸存者(27.9%)因经济原因报告处方药使用有任何变化的可能性均高于无癌症病史者(21.4%),既往确诊幸存者中各项指标的额外百分比变化范围为3.5%至9.9%,近期确诊幸存者中为2.6%至2.7%(P <.01)。老年癌症幸存者和无癌症病史者因经济原因导致处方药使用变化的发生率相当。
非老年癌症幸存者因经济原因在处方药使用变化方面特别脆弱,这表明需要有针对性的努力。《癌症》2017年;123:1453 - 1463。©2016美国癌症协会。