Patel Amisha, Mohanan P P, Prabhakaran Dorairaj, Huffman Mark D
Departments of Preventive Medicine and Medicine-Cardiology, Northwestern University Feinberg School of Medicine, Chicago, USA.
Westfort Hi-Tech Hospital, Thrissur, India.
Indian Heart J. 2017 Jan-Feb;69(1):93-100. doi: 10.1016/j.ihj.2016.07.011. Epub 2016 Jul 19.
Ischemic heart disease is the leading cause of death in India. Many of these deaths are due to acute coronary syndromes (ACS), which require prompt symptom recognition, care-seeking behavior, and transport to a treatment facility in the critical pre-hospital period. In India, little is known about pre-hospital management of individuals with ACS. We aim to understand the facilitators, barriers, and context of optimal pre-hospital ACS care to provide opportunities to reduce pre-hospital delays and improve acute cardiovascular care.
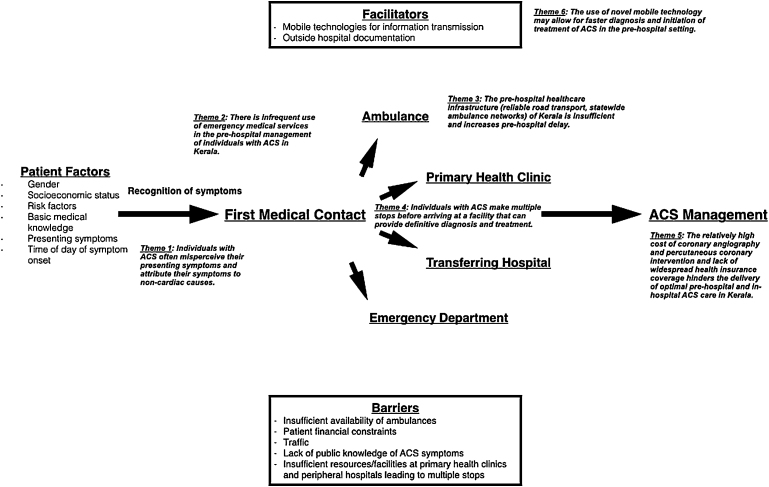
We conducted a qualitative study using in-depth interviews and focus group discussions with 27 ACS providers in Kerala, India to understand facilitators, barriers, and context to pre-hospital ACS care. Six themes emerged from these interviews and discussions: (1) individuals with ACS misperceive their symptoms as non-cardiac in origin; (2) emergency medical services are infrequently used; (3) insufficient pre-hospital healthcare infrastructure contributes to pre-hospital delay; (4) multiple stops are made before arriving at a facility that can provide definitive diagnosis and treatment; (5) relatively high costs of treatment and lack of widespread health insurance coverage limits care delivery; and (6) novel mobile technologies may allow for faster diagnosis and initiation of treatment in the pre-hospital setting.
Individualized patient-based factors (general knowledge of ACS symptoms, socioeconomic position) and broader systems-based factors (ambulance networks, coordination of transport) affect pre-hospital ACS care in Kerala. Improving public awareness of ACS symptoms, increasing appropriate use of emergency medical services, and building a infrastructure for rapid and coordinated transport may improve pre-hospital ACS care.
缺血性心脏病是印度的主要死因。其中许多死亡是由急性冠状动脉综合征(ACS)导致的,这需要在院前关键时期迅速识别症状、寻求医疗行为并转运至治疗机构。在印度,对于ACS患者的院前管理知之甚少。我们旨在了解优化院前ACS护理的促进因素、障碍和背景情况,以便找到减少院前延误并改善急性心血管护理的机会。
我们在印度喀拉拉邦对27名ACS医护人员进行了深入访谈和焦点小组讨论,以了解院前ACS护理的促进因素、障碍和背景情况。这些访谈和讨论得出了六个主题:(1)ACS患者将其症状错误地认为是非心脏源性的;(2)很少使用紧急医疗服务;(3)院前医疗基础设施不足导致院前延误;(4)在抵达能够提供明确诊断和治疗的机构之前要多次停留;(5)治疗费用相对较高且缺乏广泛的医疗保险覆盖范围限制了医疗服务的提供;(6)新型移动技术可能允许在院前环境中更快地进行诊断和开始治疗。
基于患者个体的因素(对ACS症状的一般了解、社会经济地位)和更广泛的基于系统的因素(救护车网络、转运协调)会影响喀拉拉邦的院前ACS护理。提高公众对ACS症状的认识、增加紧急医疗服务的合理使用以及建立快速协调转运的基础设施可能会改善院前ACS护理。