Miyamoto Kyohei, Kawazoe Yu, Kato Seiya
Department of Emergency and Critical Care Medicine, Wakayama Medical University, 811-1, Kimiidera, Wakayama City, Wakayama Japan.
Division of Emergency and Critical Care Medicine, Tohoku University Hospital Emergency Center, 1-1, Seiryo-machi, Aoba-ku, Sendai City, Miyagi Japan.
J Intensive Care. 2017 Feb 20;5:19. doi: 10.1186/s40560-017-0214-3. eCollection 2017.
Direct hemoperfusion therapy with polymyxin B immobilized fiber cartridges (PMX-DHP) is widely used for septic shock in Japan and parts of Europe. Although this treatment is usually administered for 2 h, the optimal duration has not been established.
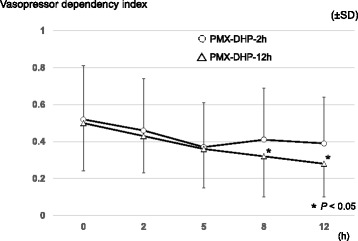
This retrospective study compared the effects of prolonged and conventional PMX-DHP durations (2 and 12 h, respectively) for septic shock. Between October 2013 and March 2015, 18 patients underwent conventional PMX-DHP, and between April 2015 and May 2016, 18 patients underwent prolonged PMX-DHP. The primary outcome was the vasopressor dependency index during the 12 h after starting the first PMX-DHP session. The vasopressor dependency index was calculated as (inotropic score)/(mean blood pressure).
The patients' characteristics were almost similar in the conventional and prolonged PMX-DHP groups. The major site of infection was the abdomen in both groups (61 and 72%, respectively). The conventional PMX-DHP group had mean blood pressure values of 68.4 ± 8.9 mmHg and 78.2 ± 16.9 mmHg at 0 and 12 h after starting PMX-DHP ( = 0.13). The prolonged PMX-DHP group had mean blood pressure values of 70.3 ± 15.7 mmHg and 87.7 ± 16.9 mmHg at 0 and 12 h after starting PMX-DHP ( = 0.004). The conventional PMX-DHP group had vasopressor dependency index values of 0.52 ± 0.29 and 0.39 ± 0.25 at 0 and 12 h after starting PMX-DHP ( = 0.29). The prolonged PMX-DHP group had vasopressor dependency index values of 0.50 ± 0.26 and 0.28 ± 0.18 at 0 and 12 h after starting PMX-DHP ( = 0.01). Hospital mortality was similar in both groups (8/18 [44%] and 8/18 [44%]).
These findings suggest that prolonged PMX-DHP provides more sustained circulatory stabilization compared to conventional PMX-DHP. However, our study failed to detect any improvement in mortality. Well-designed prospective trials are needed to examine the clinical outcomes of prolonged PMX-DHP and to identify the optimal duration of PMX-DHP.
使用多粘菌素B固定化纤维柱的直接血液灌流疗法(PMX-DHP)在日本和欧洲部分地区被广泛用于治疗感染性休克。尽管这种治疗通常进行2小时,但最佳治疗时长尚未确定。
这项回顾性研究比较了延长PMX-DHP时长(12小时)和传统时长(2小时)治疗感染性休克的效果。2013年10月至2015年3月期间,18例患者接受了传统PMX-DHP治疗;2015年4月至2016年5月期间,18例患者接受了延长PMX-DHP治疗。主要结局指标是首次进行PMX-DHP治疗后12小时内的血管升压药依赖指数。血管升压药依赖指数的计算方法为(肌力评分)/(平均血压)。
传统PMX-DHP组和延长PMX-DHP组患者的特征几乎相似。两组感染的主要部位均为腹部(分别为61%和72%)。传统PMX-DHP组在开始PMX-DHP治疗后0小时和12小时的平均血压值分别为68.4±8.9 mmHg和78.2±16.9 mmHg(P = 0.13)。延长PMX-DHP组在开始PMX-DHP治疗后0小时和12小时的平均血压值分别为70.3±15.7 mmHg和87.7±16.9 mmHg(P = 0.004)。传统PMX-DHP组在开始PMX-DHP治疗后0小时和12小时的血管升压药依赖指数值分别为0.52±0.29和0.39±0.25(P = 0.29)。延长PMX-DHP组在开始PMX-DHP治疗后0小时和12小时的血管升压药依赖指数值分别为0.50±0.26和0.28±0.18(P = 0.01)。两组的医院死亡率相似(分别为8/18 [44%]和8/18 [44%])。
这些结果表明,与传统PMX-DHP相比,延长PMX-DHP能使循环更持久地稳定。然而,我们的研究未能发现死亡率有任何改善。需要设计完善的前瞻性试验来研究延长PMX-DHP的临床结局,并确定PMX-DHP的最佳治疗时长。