Brodszky Valentin, Bíró Anikó, Szekanecz Zoltán, Soós Boglárka, Baji Petra, Rencz Fanni, Tóthfalusi László, Gulácsi László, Péntek Márta
Department of Health Economics, Corvinus University of Budapest, Budapest, Hungary.
Department of Health Economics, Corvinus University of Budapest, Budapest, Hungary; School of Economics, The University of Edinburgh, Edinburgh, UK.
Clinicoecon Outcomes Res. 2017 Feb 15;9:139-147. doi: 10.2147/CEOR.S124381. eCollection 2017.
To compare drug survival of biological therapies in patients with rheumatoid arthritis (RA), and analyze the determinants of discontinuation probabilities and switches to other biological therapies.
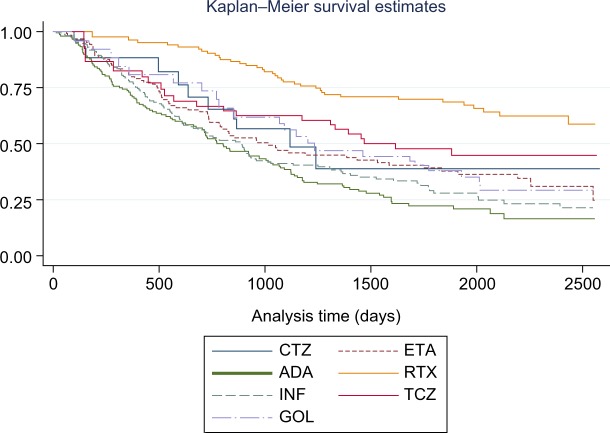
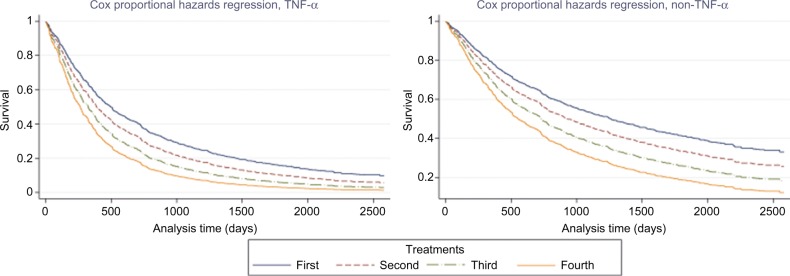
Consecutive RA patients initiating first biological treatment in one rheumatology center between 2006 and 2013 were included. Log-rank test was used to analyze the differences between the survival curves of different biological drugs. Cox regression was applied to analyze the discontinuation due to inefficacy, the occurrence of adverse events, or to any reasons.
A total of 540 patients were included in the analysis. The most frequently used first-line biological treatments were infliximab (N=176, 33%), adalimumab (N=150, 28%), and etanercept (N=132, 24%). Discontinuation of first tumor necrosis factor-alpha (TNF-α) treatment was observed for 347 (64%) patients, due to inefficacy (n=209, 60%), adverse events (n=103, 30%), and other reasons (n=35, 10%). Drug survival rates for TNF-α and non-TNF-α therapies were significantly different, and were in favor of non-TNF-α therapies. Every additional number of treatment significantly increased the risk of inefficacy by 27% (<0.001) and of adverse events by 35% (=0.002). After the discontinuation of the initial TNF-α treatment, switching to rituximab and tocilizumab was associated with significantly longer treatment duration than switching to a second TNF-α. The non-TNF-α therapies resulted in significantly longer treatment duration, due to both less adverse events and longer maintenance of effectiveness.
Non-TNF-α therapies resulted in significantly longer treatment duration, and lost their effectiveness later. Increase in the number of switches significantly increased the risk of discontinuation of any biological therapy.
比较类风湿关节炎(RA)患者生物治疗的药物留存率,并分析停药概率的决定因素以及转用其他生物治疗的情况。
纳入2006年至2013年间在一个风湿病中心开始首次生物治疗的连续RA患者。采用对数秩检验分析不同生物药物生存曲线之间的差异。应用Cox回归分析因疗效不佳、不良事件或任何原因导致的停药情况。
共540例患者纳入分析。最常用的一线生物治疗药物为英夫利昔单抗(N = 176,33%)、阿达木单抗(N = 150,28%)和依那西普(N = 132,24%)。347例(64%)患者首次肿瘤坏死因子-α(TNF-α)治疗停药,原因包括疗效不佳(n = 209,60%)、不良事件(n = 103,30%)和其他原因(n = 35,10%)。TNF-α和非TNF-α治疗的药物留存率有显著差异,非TNF-α治疗更具优势。每增加一次治疗,疗效不佳的风险显著增加27%(<0.001),不良事件风险增加35%(=0.002)。初始TNF-α治疗停药后,转用利妥昔单抗和托珠单抗的治疗持续时间显著长于转用第二种TNF-α。非TNF-α治疗导致治疗持续时间显著更长,原因是不良事件较少且疗效维持时间更长。
非TNF-α治疗导致治疗持续时间显著更长,且疗效丧失更晚。换药次数增加显著增加了任何生物治疗停药的风险。