Kantarjian Hagop, Stein Anthony, Gökbuget Nicola, Fielding Adele K, Schuh Andre C, Ribera Josep-Maria, Wei Andrew, Dombret Hervé, Foà Robin, Bassan Renato, Arslan Önder, Sanz Miguel A, Bergeron Julie, Demirkan Fatih, Lech-Maranda Ewa, Rambaldi Alessandro, Thomas Xavier, Horst Heinz-August, Brüggemann Monika, Klapper Wolfram, Wood Brent L, Fleishman Alex, Nagorsen Dirk, Holland Christopher, Zimmerman Zachary, Topp Max S
From the Department of Leukemia, University of Texas M.D. Anderson Cancer Center, Houston (H.K.); City of Hope National Medical Center, Duarte (A.S.), and Amgen, Thousand Oaks (A.F., D.N., Z.Z.) - both in California; Goethe University, University Hospital, Department of Medicine II, Frankfurt am Main (N.G.), Medical Department II (H.-A.H., M.B.) and Hematopathology Section and Lymph Node Registry (W.K.), University Hospital Schleswig Holstein, Campus Kiel, Kiel, and Medizinische Klinik und Poliklinik II, Universitätsklinikums Würzburg, Würzburg (M.S.T.) - all in Germany; Royal Free Hospital and University College London Cancer Institute, London (A.K.F.); Princess Margaret Cancer Centre, Toronto (A.C.S.), and Centre Intégré Universitaire de Santé et de Services Sociaux de l'est de l'île de Montréal, Hôpital Maisonneuve-Rosemont, Montreal (J.B.) - all in Canada; ICO-Hospital Universitari Germans Trias i Pujol, Jose Carreras Research Institute, Universitat Autonoma de Barcelona, Barcelona (J.-M.R.), the Department of Medicine, Hospital Universitari i Politecnic La Fe, University of Valencia, Valencia, and Centro de Investigación Biomédica en Red de Cáncer, Instituto Carlos III, Madrid (M.A.S.) - all in Spain; Alfred Hospital and Monash University, Melbourne, VIC, Australia (A.W.); Institut Universitaire d'Hématologie, Hôpital Saint-Louis (Assistance Publique - Hôpitaux de Paris), Paris (H.D.), and Centre Hospitalier Lyon Sud, Pierre-Benite (X.T.) - both in France; Ematologia, Dipartimento di Biotecnologie Cellulari ed Ematologia, Azienda Ospedaliera Policlinico Umberto I, Università Sapienza di Roma, Rome (R.F.), Azienda Unità Locale Socio Sanitaria 12 Veneziana Ospedale Dell Angelo, Venice (R.B.), and Azienda Socio Sanitaria Territoriale Papa Giovanni XXIII, Bergamo, Università Statale di Milano, Milan (A.R.) - all in Italy; Ankara Universitesi, Tip Fakültesi, Cebeci Arastirma ve Uygulama Hastanesi, Ankara (Ö.A.), and Dokuz Eylül Üniversitesi Tıp Fakültesi, İzmir (F.D.) - both in Turkey; Instytut Hematologii i Transfuzjologii and Centrum Medyczne Kształcenia Podyplomowego, Warsaw, Poland (E.L.-M.); University of Washington Medical Center, Seattle (B.L.W.); and Amgen, Washington, DC (C.H.).
N Engl J Med. 2017 Mar 2;376(9):836-847. doi: 10.1056/NEJMoa1609783.
Blinatumomab, a bispecific monoclonal antibody construct that enables CD3-positive T cells to recognize and eliminate CD19-positive acute lymphoblastic leukemia (ALL) blasts, was approved for use in patients with relapsed or refractory B-cell precursor ALL on the basis of single-group trials that showed efficacy and manageable toxic effects.
In this multi-institutional phase 3 trial, we randomly assigned adults with heavily pretreated B-cell precursor ALL, in a 2:1 ratio, to receive either blinatumomab or standard-of-care chemotherapy. The primary end point was overall survival.
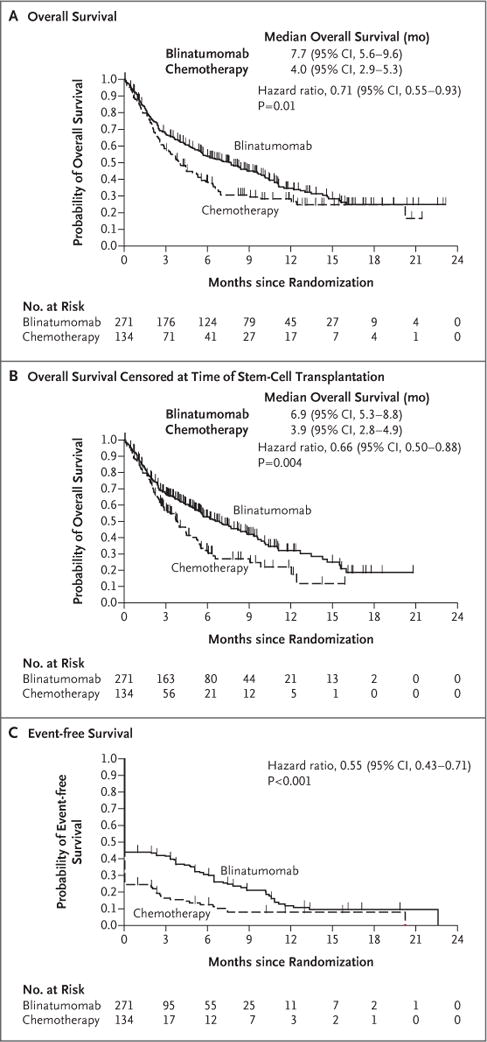
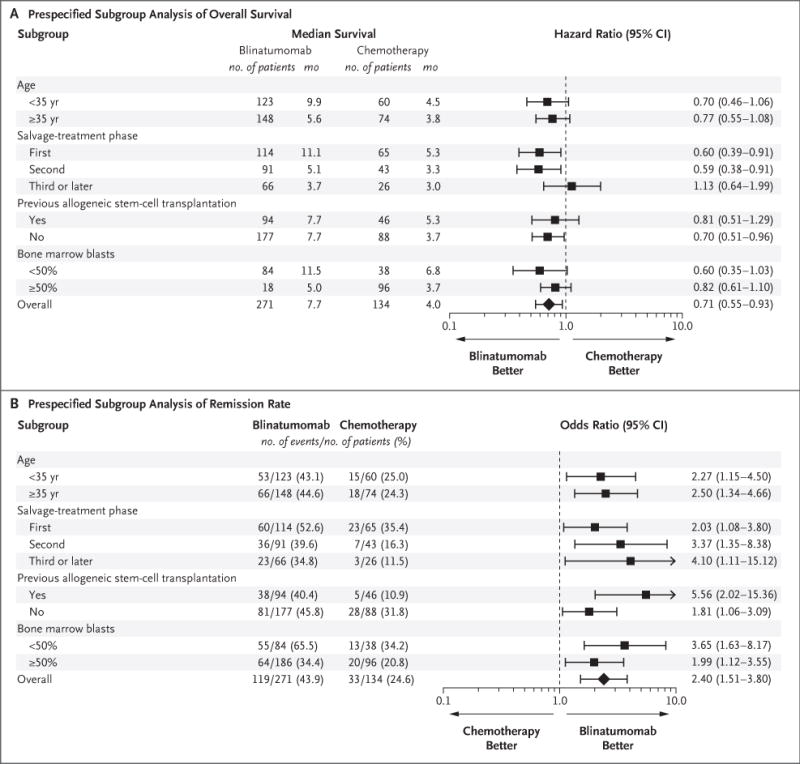
Of the 405 patients who were randomly assigned to receive blinatumomab (271 patients) or chemotherapy (134 patients), 376 patients received at least one dose. Overall survival was significantly longer in the blinatumomab group than in the chemotherapy group. The median overall survival was 7.7 months in the blinatumomab group and 4.0 months in the chemotherapy group (hazard ratio for death with blinatumomab vs. chemotherapy, 0.71; 95% confidence interval [CI], 0.55 to 0.93; P=0.01). Remission rates within 12 weeks after treatment initiation were significantly higher in the blinatumomab group than in the chemotherapy group, both with respect to complete remission with full hematologic recovery (34% vs. 16%, P<0.001) and with respect to complete remission with full, partial, or incomplete hematologic recovery (44% vs. 25%, P<0.001). Treatment with blinatumomab resulted in a higher rate of event-free survival than that with chemotherapy (6-month estimates, 31% vs. 12%; hazard ratio for an event of relapse after achieving a complete remission with full, partial, or incomplete hematologic recovery, or death, 0.55; 95% CI, 0.43 to 0.71; P<0.001), as well as a longer median duration of remission (7.3 vs. 4.6 months). A total of 24% of the patients in each treatment group underwent allogeneic stem-cell transplantation. Adverse events of grade 3 or higher were reported in 87% of the patients in the blinatumomab group and in 92% of the patients in the chemotherapy group.
Treatment with blinatumomab resulted in significantly longer overall survival than chemotherapy among adult patients with relapsed or refractory B-cell precursor ALL. (Funded by Amgen; TOWER ClinicalTrials.gov number, NCT02013167 .).
博纳吐单抗是一种双特异性单克隆抗体构建体,可使CD3阳性T细胞识别并清除CD19阳性急性淋巴细胞白血病(ALL)母细胞,基于显示出疗效和可控制毒性作用的单组试验,其被批准用于复发或难治性B细胞前体ALL患者。
在这项多机构3期试验中,我们将经过大量预处理的B细胞前体ALL成年患者按2:1的比例随机分配,分别接受博纳吐单抗或标准护理化疗。主要终点是总生存期。
在随机分配接受博纳吐单抗(271例患者)或化疗(134例患者)的405例患者中,376例患者接受了至少一剂治疗。博纳吐单抗组的总生存期显著长于化疗组。博纳吐单抗组的中位总生存期为7.7个月,化疗组为4.0个月(博纳吐单抗与化疗相比的死亡风险比为0.71;95%置信区间[CI]为0.55至0.93;P = 0.01)。治疗开始后12周内的缓解率,博纳吐单抗组显著高于化疗组,无论是完全缓解伴血液学完全恢复(34%对16%,P<0.001),还是完全缓解伴完全、部分或不完全血液学恢复(44%对25%,P<0.001)。博纳吐单抗治疗导致的无事件生存期发生率高于化疗(6个月估计值,31%对12%;在完全、部分或不完全血液学恢复后达到完全缓解后复发事件或死亡的风险比为0.55;95%CI为0.43至0.71;P<0.001),以及更长的中位缓解持续时间(7.3对4.6个月)。每个治疗组中共有24%的患者接受了异基因干细胞移植。博纳吐单抗组87%的患者和化疗组92%的患者报告了3级或更高等级的不良事件。
在复发或难治性B细胞前体ALL成年患者中,博纳吐单抗治疗导致的总生存期显著长于化疗。(由安进公司资助;TOWER临床试验注册号,NCT02013167。)