Eguchi Yawara, Toyoguchi Toru, Koda Masao, Suzuki Munetaka, Yamanaka Hajime, Tamai Hiroshi, Kobayashi Tatsuya, Orita Sumihisa, Yamauchi Kazuyo, Suzuki Miyako, Inage Kazuhide, Fujimoto Kazuki, Kanamoto Hirohito, Abe Koki, Aoki Yasuchika, Takahashi Kazuhisa, Ohtori Seiji
Department of Orthopeadic Surgery, Shimoshizu National Hospital, 934-5, Shikawatashi, Yotsukaido, Chiba 284-0003 Japan.
Department of Orthopaedic Surgery, Chiba Qiball Clinic, 4-5-1, Chuo-ku, Chiba, 260-0013 Japan.
Scoliosis Spinal Disord. 2017 Feb 22;12:5. doi: 10.1186/s13013-017-0110-6. eCollection 2017.
Age-related sarcopenia may cause physical dysfunction. We investigated the involvement of sarcopenia in dropped head syndrome (DHS).
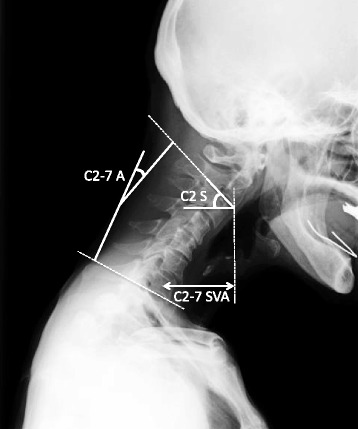
Our study subjects were ten elderly women with idiopathic DHS (mean age 75.1 years, range 55-89). Twenty age- and sex-matched volunteers (mean age 73.0, range 58-83) served as controls. We used a bioelectrical impedance analyzer (BIA) to analyze body composition, including appendicular skeletal muscle mass index (SMI; appendicular lean mass (kg)/(height (m))). SMI <5.75 was considered diagnostic for sarcopenia. Cervical sagittal plane alignment: C2-7 sagittal vertical axis (SVA), C2-7 angle (C2-C7 A), and C2 slope (C2S) were also measured. We investigated sarcopenia prevalence in both groups, height, weight, BMI, lean mass arm, lean mass leg, lean mass trunk, appendicular lean mass, total lean mass, and SMI. In addition, we also examined the correlation between cervical spine alignment and SMI in DHS.
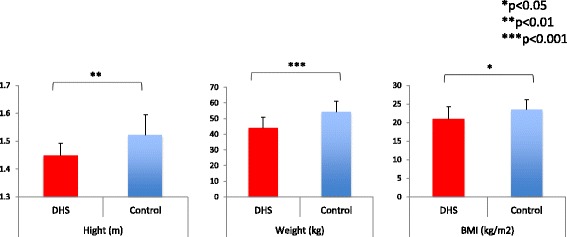
Sarcopenia was observed at a high rate in DHS subjects: 70% compared to 25% of healthy controls. Height, weight, BMI, lean mass arm, lean mass leg, axial lean mass, appendicular lean mass, total lean mass, and SMI all had significantly lower values in the DHS group. In particular, total lean mass, lean mass arm, and lean mass trunk were considerably lower in the DHS group. There was no correlation noted between cervical spine alignment and SMI.
Sarcopenia prevalence was high in the DHS group-70 versus 25% in the control group, suggesting the involvement of sarcopenia in DHS. In particular, axial lean mass and lean mass arm were markedly reduced in the DHS group. DHS is due to significant weakness of the neck extensor group, and chin-on-chest deformity occurs. Until the present, evaluation of DHS has been done using only MRI; no studies have systematically examined skeletal muscle mass. In the present study, muscle mass decrease was noted not only in the neck muscles but also throughout the entire body. Involvement of trunk and upper limb muscles in particular suggests a disuse atrophy of the upper body and spinal muscles. BIA can easily and systemically evaluate skeletal muscle mass. We expect it to contribute to further elucidating the pathogenesis of DHS.
与年龄相关的肌肉减少症可能导致身体功能障碍。我们研究了肌肉减少症与低头综合征(DHS)的关系。
我们的研究对象为10名患有特发性DHS的老年女性(平均年龄75.1岁,范围55 - 89岁)。20名年龄和性别匹配的志愿者(平均年龄73.0岁,范围58 - 83岁)作为对照。我们使用生物电阻抗分析仪(BIA)分析身体成分,包括四肢骨骼肌质量指数(SMI;四肢瘦体重(kg)/(身高(m))²)。SMI <5.75被认为是肌肉减少症的诊断标准。还测量了颈椎矢状面排列:C2 - 7矢状垂直轴(SVA)、C2 - 7角(C2 - C7 A)和C2斜率(C2S)。我们调查了两组的肌肉减少症患病率、身高、体重、体重指数、手臂瘦体重、腿部瘦体重、躯干瘦体重、四肢瘦体重、总瘦体重和SMI。此外,我们还检查了DHS患者颈椎排列与SMI之间的相关性。
DHS患者中肌肉减少症的发生率很高:为70%,而健康对照组为25%。DHS组的身高、体重、体重指数、手臂瘦体重、腿部瘦体重、轴向瘦体重、四肢瘦体重、总瘦体重和SMI的值均显著较低。特别是,DHS组的总瘦体重、手臂瘦体重和躯干瘦体重明显更低。未发现颈椎排列与SMI之间存在相关性。
DHS组的肌肉减少症患病率很高——70%,而对照组为25%,这表明肌肉减少症与DHS有关。特别是,DHS组的轴向瘦体重和手臂瘦体重明显减少。DHS是由于颈部伸肌组明显无力,导致出现低头畸形。到目前为止,对DHS的评估仅使用磁共振成像;尚无研究系统地检查骨骼肌质量。在本研究中,不仅颈部肌肉,而且全身的肌肉质量都有所下降。特别是躯干和上肢肌肉的受累表明上身和脊柱肌肉存在废用性萎缩。BIA可以轻松、系统地评估骨骼肌质量。我们期望它有助于进一步阐明DHS的发病机制。