Nieschlag Eberhard, Bouloux Pierre-Marc G, Stegmann Barbara J, Shankar R Ravi, Guan Yanfen, Tzontcheva Anjela, McCrary Sisk Christine, Behre Hermann M
University Hospital of Muenster, Center of Reproductive Medicine and Andrology, Domagkstraße 11, D-48149, Muenster, Germany.
The Royal Free Hospital, Pond St, London, NW3 2QG, UK.
Reprod Biol Endocrinol. 2017 Mar 7;15(1):17. doi: 10.1186/s12958-017-0232-y.
Hypogonadotropic hypogonadism (HH) in men results in insufficient testicular function and deficiencies in testosterone and spermatogenesis. Combinations of human chorionic gonadotropin (hCG) and recombinant follicle-stimulating hormone (recFSH) have been successful in the treatment of HH. Corifollitropin alfa is a long-acting FSH-analog with demonstrated action in women seeking infertility care. The aim of this study was to investigate the efficacy and safety of corifollitropin alfa combined with hCG to increase testicular volume and induce spermatogenesis in men with HH.
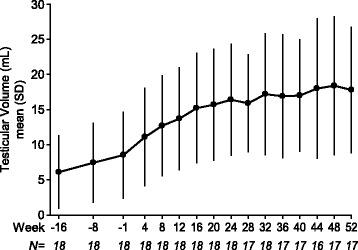
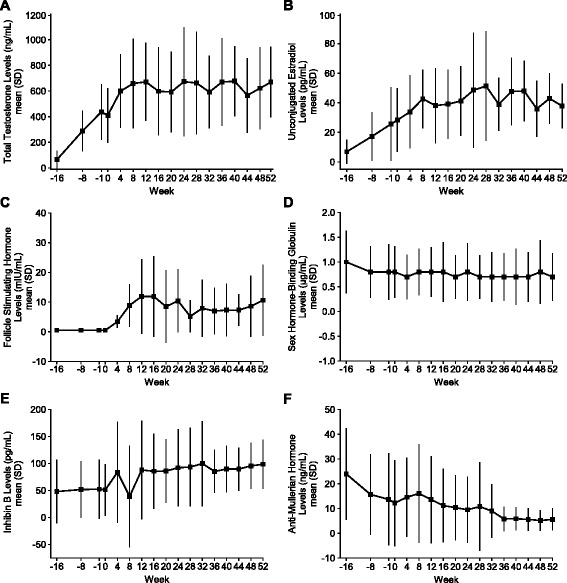
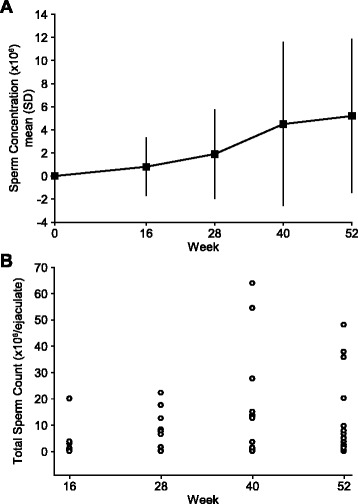
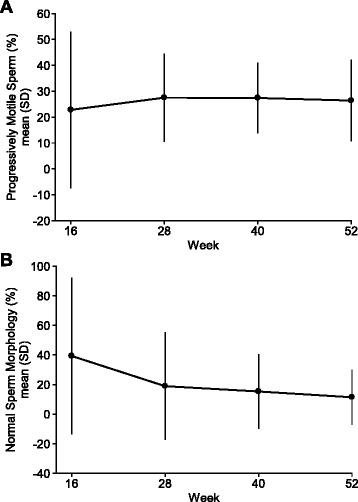
This was a Phase III, multi-center, open-label, single-arm trial of corifollitropin alfa in azoospermic men aged 18 to 50 years with HH. After 16 weeks of pretreatment of 23 subjects with hCG alone, 18 subjects with normalized testosterone (T) levels who remained azoospermic entered the 52-week combined treatment phase with hCG twice-weekly and 150 μg corifollitropin alfa every other week. The increase in testicular volume (primary efficacy endpoint) and induction of spermatogenesis resulting in a sperm count ≥1 × 10/mL (key secondary efficacy endpoint) during 52 weeks of combined treatment were assessed. Safety was evaluated by the presence of anti-corifollitropin alfa antibodies and the occurrence of adverse events (AEs).
Mean (±SD) testicular volume increased from 8.6 (±6.09) mL to 17.8 (±8.93) mL (geometric mean fold increase, 2.30 [95% CI: 2.03, 2.62]); 14 (77.8%) subjects reached a sperm count ≥1 × 10/mL. No subject developed confirmed anti-corifollitropin alfa antibodies during the trial. Treatment was generally well tolerated.
Corifollitropin alfa 150 μg administrated every other week combined with twice-weekly hCG for 52 weeks increased testicular volume significantly, and induced spermatogenesis in >75% of men with HH who had remained azoospermic after hCG treatment alone.
ClinicalTrials.gov: NCT01709331 .
男性低促性腺激素性性腺功能减退(HH)会导致睾丸功能不足以及睾酮和精子发生缺陷。人绒毛膜促性腺激素(hCG)和重组促卵泡生成素(recFSH)联合使用已成功用于治疗HH。注射用重组促卵泡素α是一种长效FSH类似物,在寻求不孕治疗的女性中已证实有作用。本研究的目的是调查注射用重组促卵泡素α联合hCG增加HH男性睾丸体积并诱导精子发生的疗效和安全性。
这是一项针对年龄在18至50岁的无精子症HH男性的注射用重组促卵泡素α的III期、多中心、开放标签、单臂试验。在23名受试者仅用hCG进行16周预处理后,18名睾酮(T)水平恢复正常但仍无精子症的受试者进入为期52周的联合治疗阶段,每周两次注射hCG,每隔一周注射150μg注射用重组促卵泡素α。评估联合治疗52周期间睾丸体积的增加(主要疗效终点)以及导致精子计数≥1×10/mL的精子发生诱导情况(关键次要疗效终点)。通过注射用重组促卵泡素α抗体的存在情况和不良事件(AE)的发生来评估安全性。
平均(±标准差)睾丸体积从8.6(±6.09)mL增加至17.8(±8.93)mL(几何平均增加倍数,2.30 [95%CI:2.03,2.62]);14名(77.8%)受试者的精子计数≥1×10/mL。在试验期间,没有受试者产生确诊的注射用重组促卵泡素α抗体。治疗总体耐受性良好。
每隔一周注射150μg注射用重组促卵泡素α并联合每周两次注射hCG共52周,可显著增加睾丸体积,并使超过75%在仅用hCG治疗后仍无精子症的HH男性诱导精子发生。
ClinicalTrials.gov:NCT01709331 。