Galey Scott A, Lerner Zachary F, Bulea Thomas C, Zimbler Seymour, Damiano Diane L
Functional & Applied Biomechanics Section, Rehabilitation Medicine Department, Clinical Center, National Institutes of Health, Bldg. 10CRC Rm 1-1469, 10 Center Dr. MSC 1604, Bethesda, MD 20892-1604, USA; The Cleveland Clinic Foundation, Cleveland, OH, USA.
Functional & Applied Biomechanics Section, Rehabilitation Medicine Department, Clinical Center, National Institutes of Health, Bldg. 10CRC Rm 1-1469, 10 Center Dr. MSC 1604, Bethesda, MD 20892-1604, USA.
Gait Posture. 2017 May;54:93-105. doi: 10.1016/j.gaitpost.2017.02.024. Epub 2017 Feb 24.
Cerebral palsy (CP) is a prevalent group of neuromotor disorders caused by early injury to brain regions or pathways that control movement. Patients with CP exhibit a range of functional motor disabilities and pathologic gait patterns. Crouch gait, characterized by increased knee flexion throughout stance, is a common gait pattern in CP that increases energy costs of walking and contributes to ambulatory decline. Our aim was to perform the first systematic literature review on the effectiveness of interventions utilized to ameliorate crouch gait in CP.
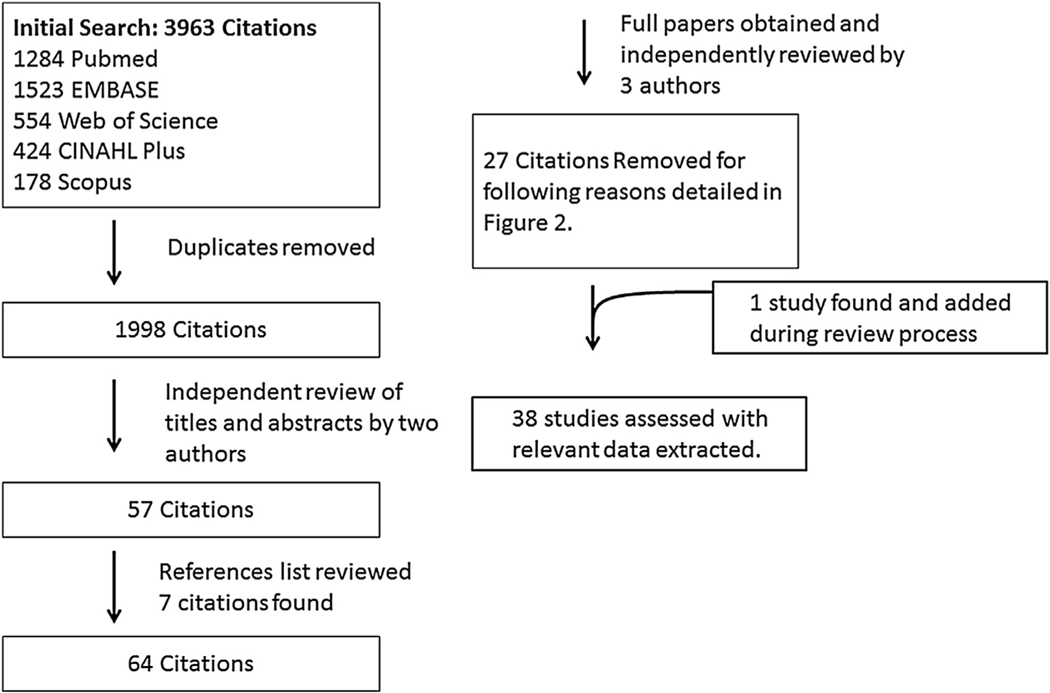
Comprehensive searches of five medical databases yielded 38 papers with 30 focused on orthopaedic management.
Evidence supports the use of initial hamstring lengthenings and rectus femoris transfers, where indicated, for improving objective gait measures with limited data on improving gait speed or gross motor function. In contrast, evidence argues against hamstring transfers and revision hamstring lengthening, with recent interest in more technically demanding corrective procedures. Only eight studies evaluated alternatives to surgery, specifically strength training, botulinum toxin or orthoses, with inconsistent and/or short-lived results.
Although crouch in CP is recognized clinically as a complex multi-joint, multi-planar gait disorder, this review largely failed to identify interventions beyond those which directly address sagittal plane knee motion, indicating a major knowledge gap. Quality of existing data was notably weak, with few studies properly controlled or adequately sized. Outcomes from specific procedures are confounded by multilevel surgeries. Successful longer term strategies to prevent worsening of crouch and subsequent functional decline are needed.
Systematic review.
脑瘫(CP)是一组常见的神经运动障碍,由控制运动的脑区或神经通路早期损伤引起。CP患者表现出一系列功能性运动障碍和病理性步态模式。蹲伏步态的特征是在整个站立期膝关节屈曲增加,是CP中常见的步态模式,会增加行走的能量消耗并导致步行能力下降。我们的目的是首次对用于改善CP患者蹲伏步态的干预措施的有效性进行系统的文献综述。
对五个医学数据库进行全面检索,得到38篇论文,其中30篇聚焦于骨科治疗。
有证据支持在有指征时使用初始的腘绳肌延长术和股直肌转移术来改善客观步态指标,但关于提高步态速度或总体运动功能的数据有限。相比之下,有证据反对腘绳肌转移术和修订的腘绳肌延长术,近期人们对技术要求更高的矫正手术感兴趣。只有八项研究评估了手术替代方案,特别是力量训练、肉毒杆菌毒素或矫形器,结果不一致和/或持续时间短。
尽管CP中的蹲伏在临床上被认为是一种复杂的多关节、多平面步态障碍,但本综述在很大程度上未能识别出除直接解决矢状面膝关节运动之外的干预措施,这表明存在重大知识空白。现有数据的质量明显较差,很少有研究进行适当的对照或有足够的样本量。特定手术的结果因多级手术而混淆。需要成功的长期策略来防止蹲伏恶化和随后的功能下降。
系统综述。