Joshi Girish P, Janis Jeffrey E, Haas Eric M, Ramshaw Bruce J, Nihira Mikio A, Dunkin Brian J
Department of Anesthesiology and Pain Management, University of Texas Southwestern Medical Center, Dallas, Tex.; Department of Plastic Surgery, Ohio State University Medical Center, Columbus, Ohio; Department of Surgery, Houston Methodist Hospital, Houston, Tex.; Department of Surgery, University of Tennessee Graduate School of Medicine, Knoxville, Tenn.; Department of Obstetrics and Gynecology and Geriatrics, University of Oklahoma College of Medicine, Oklahoma City, Okla.; and Department of Surgery, Houston Methodist Institute for Technology, Innovation, and Education, Houston, Tex.
Plast Reconstr Surg Glob Open. 2016 Dec 23;4(12):e1181. doi: 10.1097/GOX.0000000000001181. eCollection 2016 Dec.
Provision of optimal postoperative analgesia should facilitate postoperative ambulation and rehabilitation. An optimal multimodal analgesia technique would include the use of nonopioid analgesics, including local/regional analgesic techniques such as surgical site local anesthetic infiltration. This article presents a novel approach to surgical site infiltration techniques for abdominal surgery based upon neuroanatomy.
Literature searches were conducted for studies reporting the neuroanatomical sources of pain after abdominal surgery. Also, studies identified by preceding search were reviewed for relevant publications and manually retrieved.
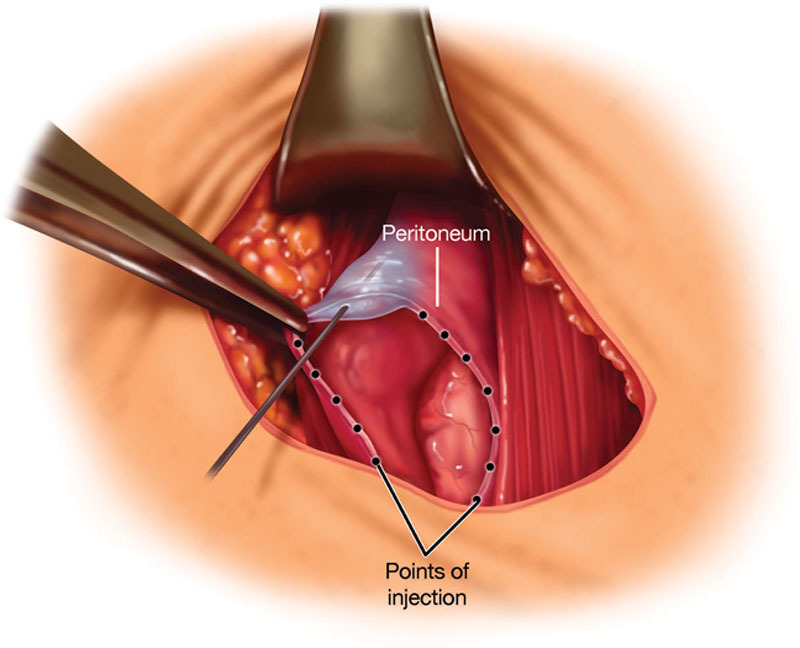
Based on neuroanatomy, an optimal surgical site infiltration technique would consist of systematic, extensive, meticulous administration of local anesthetic into the peritoneum (or preperitoneum), subfascial, and subdermal tissue planes. The volume of local anesthetic would depend on the size of the incision such that 1 to 1.5 mL is injected every 1 to 2 cm of surgical incision per layer. It is best to infiltrate with a 22-gauge, 1.5-inch needle. The needle is inserted approximately 0.5 to 1 cm into the tissue plane, and local anesthetic solution is injected while slowly withdrawing the needle, which should reduce the risk of intravascular injection.
Meticulous, systematic, and extensive surgical site local anesthetic infiltration in the various tissue planes including the peritoneal, musculofascial, and subdermal tissues, where pain foci originate, provides excellent postoperative pain relief. This approach should be combined with use of other nonopioid analgesics with opioids reserved for rescue. Further well-designed studies are necessary to assess the analgesic efficacy of the proposed infiltration technique.
提供最佳的术后镇痛应有助于术后活动和康复。一种最佳的多模式镇痛技术应包括使用非阿片类镇痛药,包括局部/区域镇痛技术,如手术部位局部麻醉药浸润。本文基于神经解剖学提出了一种腹部手术手术部位浸润技术的新方法。
对报告腹部手术后疼痛神经解剖学来源的研究进行文献检索。此外,对先前检索确定的研究进行相关出版物审查并手动检索。
基于神经解剖学,一种最佳的手术部位浸润技术应包括将局部麻醉药系统、广泛、细致地注入腹膜(或腹膜前)、筋膜下和皮下组织平面。局部麻醉药的用量取决于切口大小,即每层每1至2厘米手术切口注射1至1.5毫升。最好使用22号、1.5英寸的针头进行浸润。将针头插入组织平面约0.5至1厘米,在缓慢拔出针头的同时注入局部麻醉药溶液,这应能降低血管内注射的风险。
在包括腹膜、肌筋膜和皮下组织等疼痛病灶起源的各个组织平面进行细致、系统和广泛的手术部位局部麻醉药浸润,可提供出色的术后疼痛缓解。这种方法应与使用其他非阿片类镇痛药相结合,将阿片类药物留作备用。需要进一步设计良好的研究来评估所提出的浸润技术的镇痛效果。