Adedokun Sulaimon T, Adekanmbi Victor T, Uthman Olalekan A, Lilford Richard J
Warwick-Centre for Applied Health Research and Delivery (WCAHRD), Division of Health Sciences, University of Warwick Medical School, Coventry, United Kingdom.
Department of Demography and Social Statistics, Obafemi Awolowo University, Ile Ife, Nigeria.
PLoS One. 2017 Mar 15;12(3):e0173578. doi: 10.1371/journal.pone.0173578. eCollection 2017.
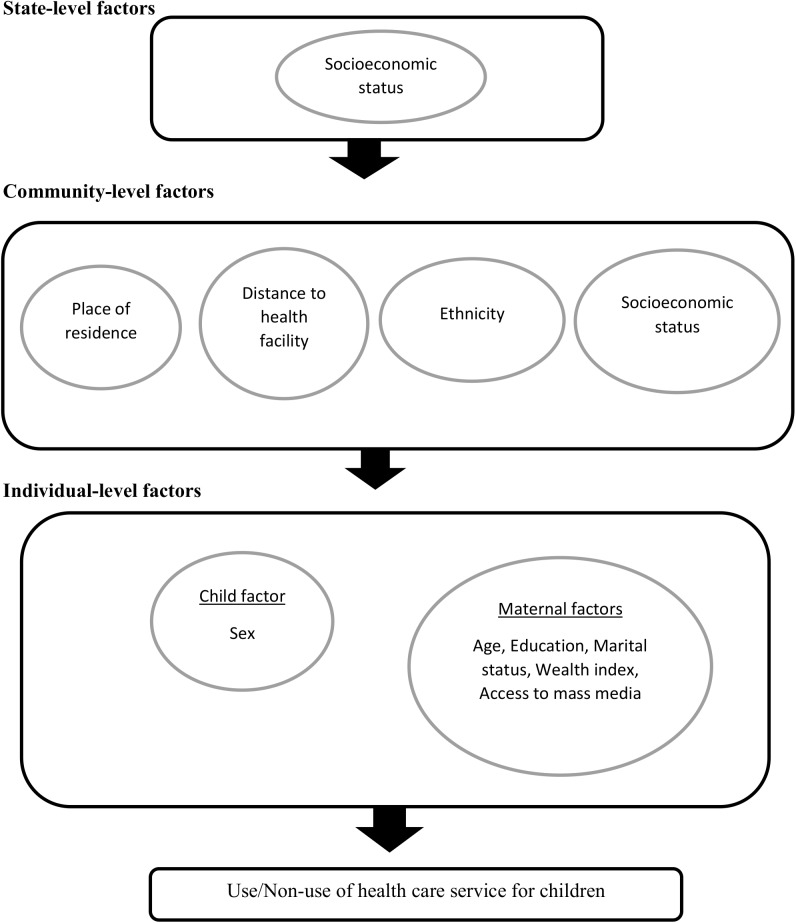
To examine the independent contribution of individual, community and state-level factors to health care service utilization for children with acute childhood illnesses in Nigeria.
The study was based on secondary analyses of cross-sectional population-based data from the 2013 Nigeria Demographic and Health Survey (DHS). Multilevel logistic regression models were applied to the data on 6,427 under-five children who used or did not use health care service when they were sick (level 1), nested within 896 communities (level 2) from 37 states (level 3).
About one-quarter of the mothers were between 15 and 24 years old and almost half of them did not have formal education (47%). While only 30% of the children utilized health service when they were sick, close to 67% lived in the rural area. In the fully adjusted model, mothers with higher education attainment (Adjusted odds ratio [aOR] = 1.63; 95% credible interval [CrI] = 1.31-2.03), from rich households (aOR = 1.76; 95% CrI = 1.35-2.25), with access to media (radio, television or magazine) (aOR = 1.18; 95% CrI = 1.08-1.29), and engaging in employment (aOR = 1.18; 95% CrI = 1.02-1.37) were significantly more likely to have used healthcare services for acute childhood illnesses. On the other hand, women who experienced difficulty getting to health facilities (aOR = 0.87; 95% CrI = 0.75-0.99) were less likely to have used health service for their children.
Our findings highlight that utilization of healthcare service for acute childhood illnesses was influenced by not only maternal factors but also community-level factors, suggesting that public health strategies should recognise this complex web of individual composition and contextual composition factors to guide provision of healthcare services. Such interventions could include: increase in female school enrolment, provision of interest-free loans for small and medium scale enterprises, introduction of mobile clinics and establishment of more primary health care centres.
探讨个体、社区和州层面因素对尼日利亚患急性儿童疾病儿童医疗服务利用情况的独立影响。
本研究基于对2013年尼日利亚人口与健康调查(DHS)中基于人群的横断面数据的二次分析。多水平逻辑回归模型应用于6427名五岁以下儿童的数据,这些儿童在生病时使用或未使用医疗服务(一级),嵌套于来自37个州的896个社区(二级)中。
约四分之一的母亲年龄在15至24岁之间,其中近一半没有受过正规教育(47%)。虽然只有30%的儿童在生病时使用了医疗服务,但近67%居住在农村地区。在完全调整模型中,受过高等教育的母亲(调整优势比[aOR]=1.63;95%可信区间[CrI]=1.31 - 2.03)、来自富裕家庭的母亲(aOR = 1.76;95% CrI = 1.35 - 2.25)、能接触到媒体(广播、电视或杂志)的母亲(aOR = 1.18;95% CrI = 1.08 - 1.29)以及有工作的母亲(aOR = 1.18;95% CrI = 1.02 - 1.37)更有可能为患急性儿童疾病的孩子使用医疗服务。另一方面,前往医疗机构有困难的女性(aOR = 0.87;95% CrI = 0.75 - 0.99)为孩子使用医疗服务的可能性较小。
我们的研究结果表明,患急性儿童疾病时医疗服务的利用不仅受到母亲因素的影响,还受到社区层面因素的影响,这表明公共卫生策略应认识到个体构成和背景构成因素的这一复杂网络,以指导医疗服务的提供。此类干预措施可包括:提高女性入学率、为中小企业提供无息贷款、引入流动诊所以及建立更多的初级卫生保健中心。