Maggiolo Franco, Gulminetti Roberto, Pagnucco Layla, Digaetano Margherita, Benatti Simone, Valenti Daniela, Callegaro Annapaola, Ripamonti Diego, Mussini Cristina
Division of Infectious Diseases, ASST Papa Giovanni XXIII, Piazza OMS 1, 24127, Bergamo, Italy.
Division of Infectious Diseases, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy.
BMC Infect Dis. 2017 Mar 16;17(1):215. doi: 10.1186/s12879-017-2311-2.
Little is known about the applicability of dual treatments based on integrase inhibitors. We explored the combination of lamivudine + dolutegravir as an option when switching from standard cART in virologically suppressed patients.
In this prospective cohort we enrolled patients previously switched to 3TC + DTG who were 18 years or older, with no previous resistance mutations to the used drugs, having a HIV-RNA <50 copies/ml for 6 months or longer, negative for HBsAg and on a stable (>6 months) cART.
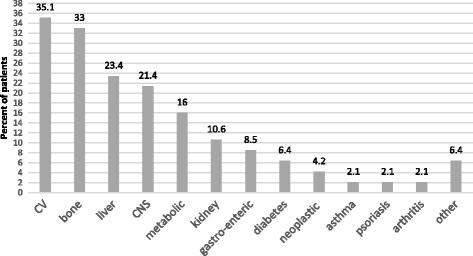
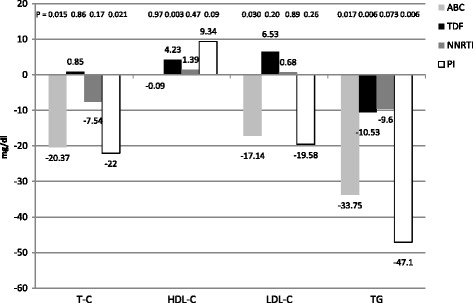
Ninety-four individuals were included. They were mostly men (77.7%) with a mean age of 53 years. They presented 159 co-morbidities including cardiovascular, bone, hepatic, kidney, and CNS diseases. Because of these pathologies, they took 207 non-ARV drugs (mean 2.2 per patient). Median duration of viral suppression was 77.5 months (IQR 61). All subjects were prospectively followed up to week 24 and all remained on dual therapy during the whole period. Neither virological failure, nor viral blip was detected. The median CD4 count rose from 658 cells/mcl (IQR 403) to 724 cells/mcl (IQR 401) (P = 0.006) without a significant (P = 0.44) change in the CD4/CD8 ratio. A significant (P < 0.0001) increment of median creatinine from 0.87 mg/dl (IQR 0.34) to 0.95 mg/dl (IQR 0.29) was observed in the first 2 months but thereafter leveled on these values (1.00 mg/dl; IQR 0.35) (P = 0.111 compared to 2 months). The lipid profile slightly improved. The daily cost of cART was significantly (P < 0.0001) reduced of 6.89 euros (SD 6.10).
Switching to a dual cART regimen based on lamivudine + dolutegravir maintains virological efficacy up to week 24, and is associated to slight improvements of the immunologic and metabolic status. The strategy allows to freely using concomitant medications for associated pathologies. The dual therapy is less expensive in economic terms.
Although still limited evidence exists, a dolutegravir-based dual therapy in combination with lamivudine shows promising results to be confirmed in larger controlled trials.
关于基于整合酶抑制剂的双重治疗的适用性知之甚少。我们探讨了在病毒学抑制的患者从标准的联合抗逆转录病毒治疗(cART)转换时,使用拉米夫定+多替拉韦作为一种选择。
在这项前瞻性队列研究中,我们纳入了年龄在18岁及以上、既往对所用药物无耐药突变、HIV-RNA<50拷贝/ml达6个月或更长时间、乙肝表面抗原阴性且接受稳定(>6个月)cART治疗、之前已转换为3TC+DTG治疗的患者。
纳入了94名个体。他们大多为男性(77.7%),平均年龄53岁。他们存在159种合并症,包括心血管、骨骼、肝脏、肾脏和中枢神经系统疾病。由于这些病症,他们服用了207种非抗逆转录病毒药物(平均每位患者2.2种)。病毒抑制的中位持续时间为77.5个月(四分位间距61)。所有受试者均接受前瞻性随访至第24周,且在整个期间均维持双重治疗。未检测到病毒学失败或病毒波动。中位CD4细胞计数从658个/微升(四分位间距403)升至724个/微升(四分位间距401)(P=0.006),而CD4/CD8比值无显著变化(P=0.44)。在最初2个月观察到肌酐中位数从0.87mg/dl(四分位间距0.34)显著增加(P<0.0001)至0.95mg/dl(四分位间距0.29),但此后稳定在这些值(1.00mg/dl;四分位间距0.35)(与2个月时相比,P=0.111)。血脂谱略有改善。cART的每日费用显著降低(P<0.0001),降低了6.89欧元(标准差6.10)。
转换为基于拉米夫定+多替拉韦的双重cART方案在第24周时维持病毒学疗效,并与免疫和代谢状态的轻微改善相关。该策略允许自由使用针对相关病症的伴随药物。从经济角度来看,双重治疗费用更低。
尽管现有证据仍然有限,但基于多替拉韦的双重治疗联合拉米夫定显示出有前景的结果,有待在更大规模的对照试验中得到证实。