Cadilhac Dominique A, Kilkenny Monique F, Andrew Nadine E, Ritchie Elizabeth, Hill Kelvin, Lalor Erin
Stroke and Ageing Research, School of Clinical Sciences at Monash Health, Department of Medicine, Monash University, Clayton, 3168, Vic, Australia.
The Florey Institute of Neuroscience and Mental Health, Stroke Division, Heidelberg, 3081, Vic, Australia.
BMC Health Serv Res. 2017 Mar 16;17(1):212. doi: 10.1186/s12913-017-2150-2.
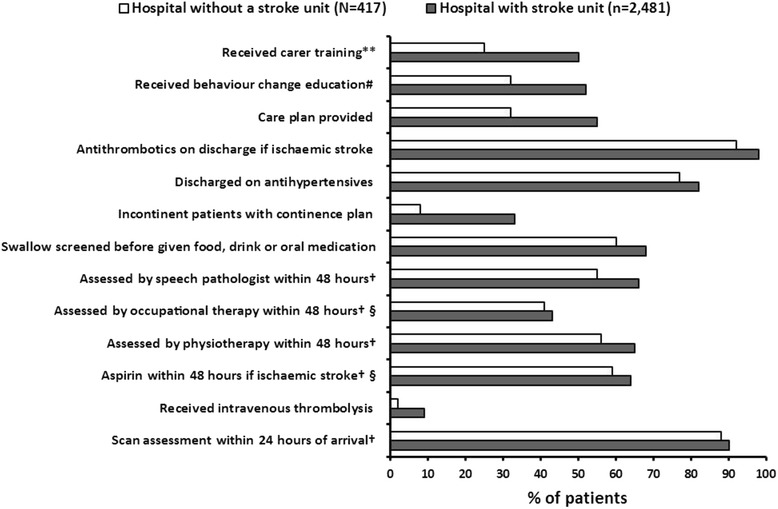
Establishing a stroke unit (SU) in every hospital may be infeasible because of limited resources. In Australia, it is recommended that hospitals that admit ≥100 strokes per year should have a SU. We aimed to describe differences in processes of care and outcomes among hospitals with and without SUs admitting at least 100 patients/year.
National stroke audit data of 40 consecutive patients per hospital admitted between 1/7/2010-31/12/2010 and organizational survey for annual admissions were used. Descriptive analyses and multilevel regression were used to compare patient outcomes. Sensitivity analysis including only hospitals meeting all of the Australian SU criteria (e.g., co-location of beds; inter-professional team; weekly meetings; regular training) was performed.
Two thousand eight hundred ninety-eight patients from 72/108 eligible hospitals completing the audit (SU = 60; patients: 2,481 [mean age 76 years; 55% male] and non-SU patients: 417 [mean age 77; 53% male]). Hospitals with SUs had greater adherence to recommended care processes than non-SU hospitals. Patients treated in a SU hospital had fewer new strokes while in hospital (OR: 0.20; 95% CI 0.06, 0.61) and there was a borderline reduction in the odds of dying in hospital compared to patients in non-SU hospitals (OR 0.57 95%CI 0.33, 1.00). Among SU hospitals meeting all SU criteria (n = 59; 91%) the adjusted odds of having a poor outcome was further reduced compared with patients attending non-SU hospitals.
Hospitals annually admitting ≥100 patients with acute stroke should be prioritized for establishment of a SU that meet all recommended criteria to ensure better outcomes.
由于资源有限,在每家医院设立卒中单元(SU)可能并不可行。在澳大利亚,建议每年收治≥100例卒中患者的医院应设立卒中单元。我们旨在描述每年收治至少100例患者的有卒中单元和无卒中单元的医院在护理流程和结局方面的差异。
使用2010年7月1日至2010年12月31日期间每家医院连续收治的40例患者的全国卒中审计数据以及年度入院情况的组织调查。采用描述性分析和多水平回归比较患者结局。进行了敏感性分析,仅纳入符合所有澳大利亚卒中单元标准(如床位集中设置;跨专业团队;每周会议;定期培训)的医院。
来自72/108家符合条件并完成审计的医院的2898例患者(卒中单元医院=60家;患者2481例[平均年龄76岁;55%为男性],非卒中单元医院患者417例[平均年龄77岁;53%为男性])。有卒中单元的医院比无卒中单元的医院更严格遵循推荐的护理流程。在卒中单元医院接受治疗的患者住院期间新发卒中较少(比值比:0.20;95%置信区间0.06,0.61),与非卒中单元医院的患者相比,住院死亡几率有临界降低(比值比0.57,95%置信区间0.33,1.00)。在符合所有卒中单元标准的卒中单元医院中(n = 59;91%),与在非卒中单元医院就诊的患者相比,不良结局的校正几率进一步降低。
每年收治≥100例急性卒中患者的医院应优先设立符合所有推荐标准的卒中单元,以确保更好的结局。