Glowka Tim R, Webler Markus, Matthaei Hanno, Schäfer Nico, Schmitz Volker, Kalff Jörg C, Standop Jens, Manekeller Steffen
Department of Surgery, University of Bonn, Sigmund-Freud-Str. 25, 53105, Bonn, Germany.
Department of Orthopedic and Trauma Surgery, University of Bonn, Sigmund-Freud-Str. 25, 53105, Bonn, Germany.
BMC Surg. 2017 Mar 20;17(1):24. doi: 10.1186/s12893-017-0226-x.
Delayed gastric emptying (DGE) remains the most frequent complication following pancreatoduodenectomy (PD) with published incidences as high as 61%. The present study investigates the impact of bowel reconstruction techniques on DGE following classic PD (Whipple-Kausch procedure) with pancreatogastrostomy (PG).
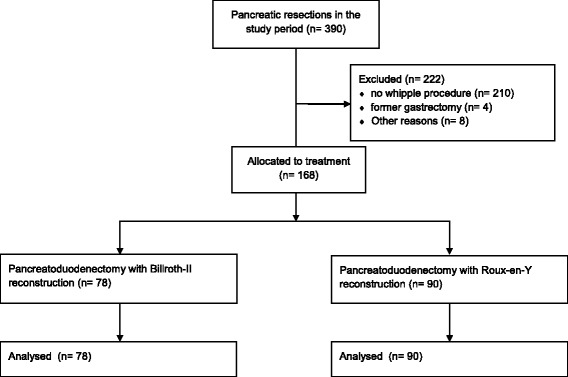
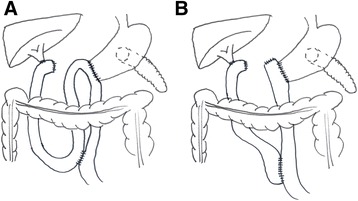
We included 168 consecutive patients who underwent PD with PG with either Billroth II type (BII, n = 78) or Roux-en-Y type reconstruction (ReY, n = 90) between 2004 and 2015. Excluded were patients with conventional single loop reconstruction after pylorus preserving procedures. DGE was classified according to the 2007 International Study Group of Pancreatic Surgery definition. Patients were analyzed regarding severity of DGE, morbidity and mortality, length of hospital stay and demographic factors.
No difference was observed between BII and ReY regarding frequency of DGE. Overall rate for clinically relevant DGE was 30% (ReY) and 26% (BII). BII and ReY did not differ in terms of demographics, morbidity or mortality. DGE significantly prolongs ICU (four vs. two days) and hospital stay (20.5 vs. 14.5 days). Risk factors for DGE development are advanced age, retrocolic reconstruction, postoperative hemorrhage and major complications.
The occurrence of DGE can not be influenced by the type of alimentary reconstruction (ReY vs. BII) following classic PD with PG. Old age and major complications could be identified as important risk factors in multivariate analysis.
German Clinical Trials Register (DRKS) DRKS00011860 . Registered 14 March 2017.
胃排空延迟(DGE)仍是胰十二指肠切除术(PD)后最常见的并发症,已发表的发生率高达61%。本研究调查了在采用胰胃吻合术(PG)的经典PD(惠普尔-考施手术)后,肠道重建技术对DGE的影响。
我们纳入了2004年至2015年间连续接受PG的PD患者168例,其中行毕罗Ⅱ式(BII,n = 78)或 Roux-en-Y 式重建(ReY,n = 90)。排除保留幽门手术后采用传统单环重建的患者。根据2007年国际胰腺手术研究组的定义对DGE进行分类。分析患者的DGE严重程度、发病率和死亡率、住院时间及人口统计学因素。
BII和ReY在DGE发生率方面未观察到差异。临床相关DGE的总体发生率为30%(ReY)和26%(BII)。BII和ReY在人口统计学、发病率或死亡率方面无差异。DGE显著延长了重症监护病房(ICU)住院时间(4天对2天)和总住院时间(20.5天对14.5天)。DGE发生的危险因素为高龄、结肠后重建、术后出血和严重并发症。
在采用PG的经典PD后,消化道重建类型(ReY与BII)不会影响DGE的发生。在多因素分析中,高龄和严重并发症可被确定为重要危险因素。
德国临床试验注册中心(DRKS)DRKS00011860。2017年3月14日注册。