Qian Jing, Wolters Frank J, Beiser Alexa, Haan Mary, Ikram M Arfan, Karlawish Jason, Langbaum Jessica B, Neuhaus John M, Reiman Eric M, Roberts J Scott, Seshadri Sudha, Tariot Pierre N, Woods Beth McCarty, Betensky Rebecca A, Blacker Deborah
Department of Biostatistics and Epidemiology, University of Massachusetts Amherst, Amherst, Massachusetts, United States of America.
Department of Epidemiology, Erasmus Medical Center, Rotterdam, the Netherlands.
PLoS Med. 2017 Mar 21;14(3):e1002254. doi: 10.1371/journal.pmed.1002254. eCollection 2017 Mar.
With the onset of prevention trials for individuals at high risk for Alzheimer disease, there is increasing need for accurate risk prediction to inform study design and enrollment, but available risk estimates are limited. We developed risk estimates for the incidence of mild cognitive impairment (MCI) or dementia among cognitively unimpaired individuals by APOE-e4 dose for the genetic disclosure process of the Alzheimer's Prevention Initiative Generation Study, a prevention trial in cognitively unimpaired APOE-e4/e4 homozygote individuals.
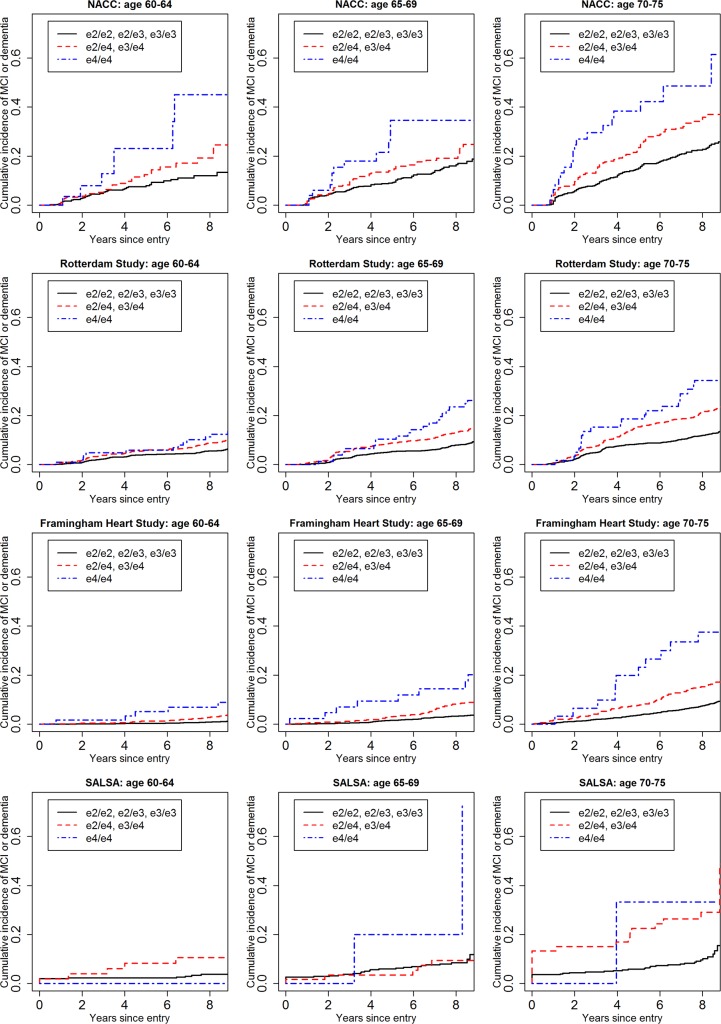
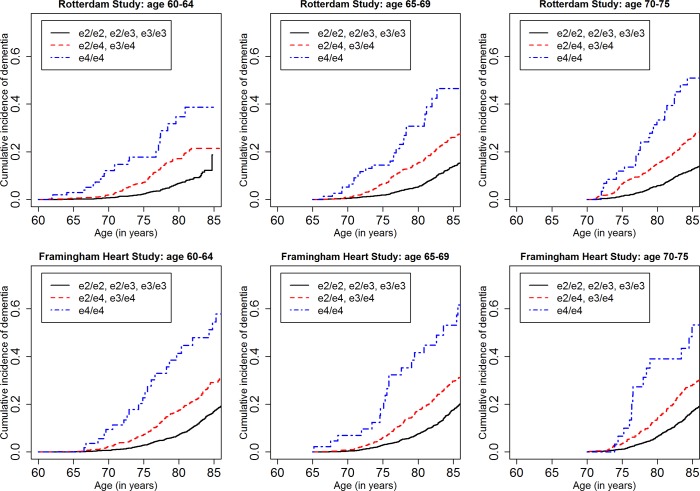
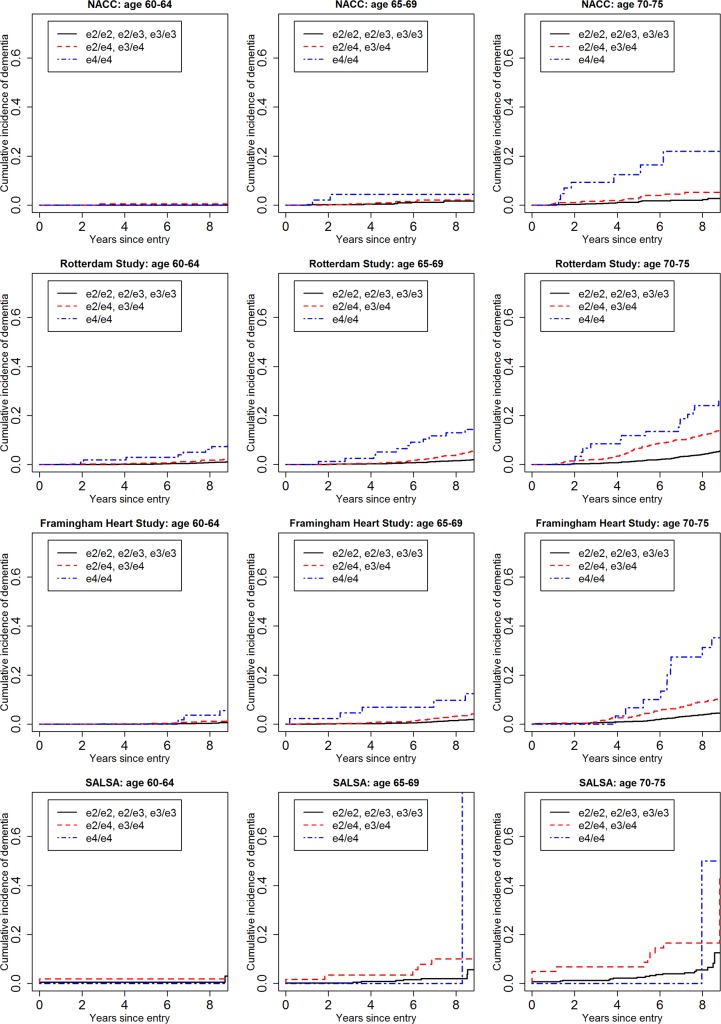
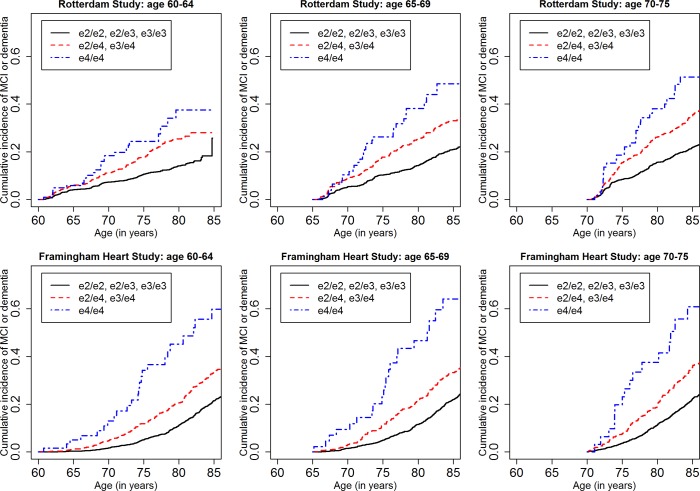
We included cognitively unimpaired individuals aged 60-75 y, consistent with Generation Study eligibility criteria, from the National Alzheimer's Coordinating Center (NACC) (n = 5,073, 158 APOE-e4/e4), the Rotterdam Study (n = 6,399, 156 APOE-e4/e4), the Framingham Heart Study (n = 4,078, 67 APOE-e4/e4), and the Sacramento Area Latino Study on Aging (SALSA) (n = 1,294, 11 APOE-e4/e4). We computed stratified cumulative incidence curves by age (60-64, 65-69, 70-75 y) and APOE-e4 dose, adjusting for the competing risk of mortality, and determined risk of MCI and/or dementia by genotype and baseline age. We also used subdistribution hazard regression to model relative hazard based on age, APOE genotype, sex, education, family history of dementia, vascular risk, subjective memory concerns, and baseline cognitive performance. The four cohorts varied considerably in age, education, ethnicity/race, and APOE-e4 allele frequency. Overall, cumulative incidence was uniformly higher in NACC than in the population-based cohorts. Among APOE-e4/e4 individuals, 5-y cumulative incidence was as follows: in the 60-64-y age stratum, it ranged from 0% to 5.88% in the three population-based cohorts versus 23.06% in NACC; in the 65-69-y age stratum, from 9.42% to 10.39% versus 34.62%; and in the 70-75-y age stratum, from 18.64% to 33.33% versus 38.34%. Five-year incidence of dementia was negligible except for APOE-e4/e4 individuals and those over 70 y. Lifetime incidence (to age 80-85 y) of MCI or dementia for the APOE-e4/e4 individuals in the long-term Framingham and Rotterdam cohorts was 34.69%-38.45% at age 60-64 y, 30.76%-40.26% at 65-69 y, and 33.3%-35.17% at 70-75 y. Confidence limits for these estimates are often wide, particularly for APOE-e4/e4 individuals and for the dementia outcome at 5 y. In regression models, APOE-e4 dose and age both consistently increased risk, as did lower education, subjective memory concerns, poorer baseline cognitive performance, and family history of dementia. We discuss several limitations of the study, including the small numbers of APOE-e4/e4 individuals, missing data and differential dropout, limited ethnic and racial diversity, and differences in definitions of exposure and outcome variables.
Estimates of the absolute risk of MCI or dementia, particularly over short time intervals, are sensitive to sampling and a variety of methodological factors. Nonetheless, such estimates were fairly consistent across the population-based cohorts, and lower than those from a convenience cohort and those estimated in prior studies-with implications for informed consent and design for clinical trials targeting high-risk individuals.
随着针对阿尔茨海默病高危个体的预防试验的开展,为研究设计和入组提供信息的准确风险预测的需求日益增加,但现有的风险估计有限。我们针对阿尔茨海默病预防计划一代研究(一项针对认知未受损的APOE - e4/e4纯合子个体的预防试验)的基因披露过程,按APOE - e4剂量计算了认知未受损个体中轻度认知障碍(MCI)或痴呆症发病率的风险估计值。
我们纳入了来自国家阿尔茨海默病协调中心(NACC)(n = 5073,158例APOE - e4/e4)、鹿特丹研究(n = 6399,156例APOE - e4/e4)、弗雷明汉心脏研究(n = 4078,67例APOE - e4/e4)以及萨克拉门托地区拉丁裔老龄化研究(SALSA)(n = 1294,11例APOE - e4/e4)的60 - 75岁认知未受损个体,这些个体符合一代研究的纳入标准。我们按年龄(60 - 64岁、65 - 69岁、70 - 75岁)和APOE - e4剂量计算分层累积发病率曲线,并对死亡的竞争风险进行调整,确定了不同基因型和基线年龄的MCI和/或痴呆症风险。我们还使用亚分布风险回归模型,根据年龄、APOE基因型、性别、教育程度、痴呆家族史、血管风险、主观记忆问题以及基线认知表现来模拟相对风险。这四个队列在年龄、教育程度、种族/民族以及APOE - e4等位基因频率方面差异很大。总体而言,NACC队列中的累积发病率始终高于基于人群的队列。在APOE - e4/e4个体中,5年累积发病率如下:在60 - 64岁年龄组,三个基于人群的队列中发病率为0%至5.88%,而NACC队列中为23.06%;在65 - 69岁年龄组,为9.42%至10.39%,而NACC队列中为34.62%;在70 - 75岁年龄组,为18.64%至33.33%,而NACC队列中为38.34%。除了APOE - e4/e4个体和70岁以上个体外,痴呆症的5年发病率可忽略不计。长期弗雷明汉和鹿特丹队列中APOE - e4/e4个体到80 - 85岁时MCI或痴呆症的终生发病率在60 - 64岁时为34.69% - 38.45%,65 - 69岁时为30.76% - 40.26%,70 - 75岁时为33.3% - 35.17%。这些估计值的置信区间通常较宽,尤其是对于APOE - e4/e4个体以及5年时的痴呆症结果。在回归模型中,APOE - e4剂量和年龄均持续增加风险,较低的教育程度、主观记忆问题、较差的基线认知表现以及痴呆家族史也增加风险。我们讨论了该研究的几个局限性,包括APOE - e4/e4个体数量较少、数据缺失和差异失访、种族和民族多样性有限以及暴露和结局变量定义的差异。
MCI或痴呆症绝对风险的估计值,尤其是在短时间间隔内,对抽样和各种方法学因素敏感。尽管如此,这些估计值在基于人群的队列中相当一致,且低于便利样本队列以及先前研究中的估计值——这对针对高危个体的临床试验的知情同意和设计具有启示意义。