Kozlowska Kasia, Rampersad Reena, Cruz Catherine, Shah Ubaid, Chudleigh Catherine, Soe Samantha, Gill Deepak, Scher Stephen, Carrive Pascal
Psychological Medicine, The Children's Hospital at Westmead, Locked Bag 4001, Westmead, NSW, 2145, Australia.
Brain Dynamics Centre, Westmead Institute for Medical Research, Westmead, NSW, Australia.
Eur Child Adolesc Psychiatry. 2017 Oct;26(10):1207-1217. doi: 10.1007/s00787-017-0976-0. Epub 2017 Mar 24.
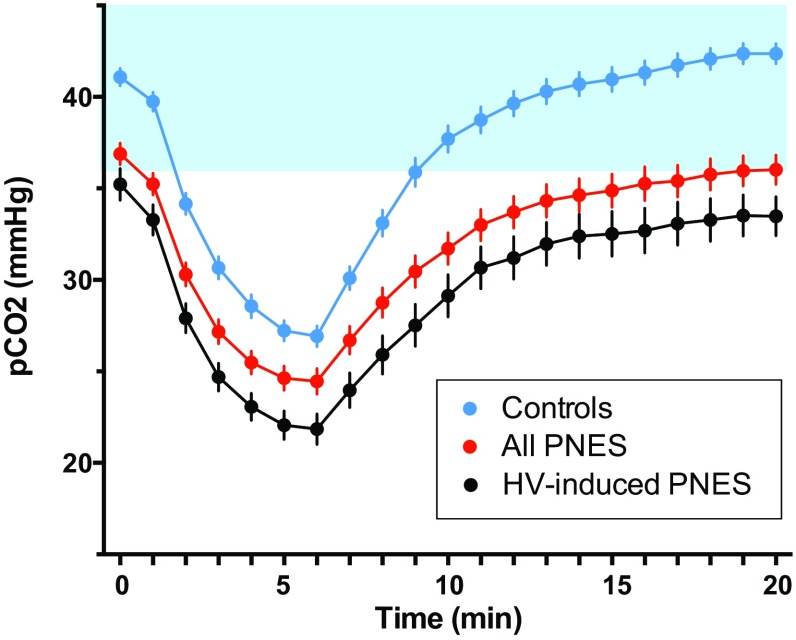
Psychogenic non-epileptic seizures (PNES) are a common problem in paediatric neurology and psychiatry that can best be understood as atypical responses to threat. Threats activate the body for action by mediating increases in arousal, respiration, and motor readiness. In previous studies, a range of cardiac, endocrine, brain-based, attention-bias, and behavioral measures have been used to demonstrate increases in arousal, vigilance, and motor readiness in patients with PNES. The current study uses respiratory measures to assess both the motor readiness of the respiratory system and the respiratory regulation of CO. Baseline respiratory rates during clinical assessment and arterial CO levels during the hyperventilation component of routine video electroencephalogram were documented in 60 children and adolescents referred for treatment of PNES and in 50 controls. Patients showed elevated baseline respiratory rates [t(78) = 3.34, p = .001], with 36/52 (69%) of patients [vs. 11/28 (39%) controls] falling above the 75th percentile (χ = 6.7343; df = 1; p = .009). Twenty-eight (47%) of patients [vs. 4/50 (8%) controls] showed a skewed hyperventilation-challenge profile-baseline PCO <36 mmHg, a trough PCO ≤ 20 mmHg, or a final PCO <36 mmHg after 15 min of recovery-signaling difficulties with CO regulation (χ = 19.77; df = 1; p < .001). Children and adolescents with PNES present in a state of readiness-for-action characterized by high arousal coupled with activation of the respiratory motor system, increases in ventilation, and a hyperventilation-challenge profile shifted downward from homeostatic range. Breathing interventions that target arousal, decrease respiratory rate, and normalize ventilation and arterial CO may help patients shift brain-body state and avert PNES episodes.
心理性非癫痫性发作(PNES)是儿科神经病学和精神病学中的常见问题,最好将其理解为对威胁的非典型反应。威胁通过介导唤醒、呼吸和运动准备状态的增加来激活身体以采取行动。在先前的研究中,一系列心脏、内分泌、基于脑、注意力偏差和行为测量方法已被用于证明PNES患者的唤醒、警觉和运动准备状态增加。本研究使用呼吸测量方法来评估呼吸系统的运动准备状态和二氧化碳的呼吸调节。在60名因PNES接受治疗的儿童和青少年以及50名对照组中,记录了临床评估期间的基线呼吸频率和常规视频脑电图过度通气部分期间的动脉二氧化碳水平。患者的基线呼吸频率升高[t(78) = 3.34, p = .001],52名患者中有36名(69%)[相比之下,28名对照组中有11名(39%)]高于第75百分位数(χ = 6.7343;自由度 = 1;p = .009)。28名(47%)患者[相比之下,50名对照组中有4名(8%)]表现出异常的过度通气挑战曲线——基线二氧化碳分压<36 mmHg、谷值二氧化碳分压≤20 mmHg或恢复15分钟后的最终二氧化碳分压<36 mmHg,表明二氧化碳调节存在困难(χ = 19.77;自由度 = 1;p < .001)。患有PNES的儿童和青少年呈现出一种准备行动的状态,其特征是高度唤醒,伴有呼吸运动系统的激活、通气增加以及过度通气挑战曲线从稳态范围向下偏移。针对唤醒、降低呼吸频率并使通气和动脉二氧化碳正常化的呼吸干预措施可能有助于患者改变脑-身状态并避免PNES发作。