Kieneker Lyanne M, Eisenga Michele F, Joosten Michel M, de Boer Rudolf A, Gansevoort Ron T, Kootstra-Ros Jenny E, Navis Gerjan, Bakker Stephan J L
Department of Internal Medicine, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands.
Department of Cardiology, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands.
PLoS One. 2017 Mar 27;12(3):e0174686. doi: 10.1371/journal.pone.0174686. eCollection 2017.
Both hypokalemia and hyperkalemia are associated with disease progression in patients with chronic kidney disease (CKD). It is unclear whether similar associations are present in the general population. Our aim was to examine the association of plasma potassium with risk of developing CKD and the role of diuretics in this association in a population-based cohort.
We studied 5,130 subjects free of CKD at baseline of the Prevention of Renal and Vascular End-Stage Disease (PREVEND) study, a prospective, population-based cohort of Dutch men and women aged 28-75 years. Hypokalemia was defined as plasma potassium <3.5 mmol/L, and hyperkalemia as plasma potassium ≥5.0 mmol/L. Risk of CKD was defined as de novo development of eGFR <60 ml/min/1.73m2 and/or albuminuria >30 mg/24h.
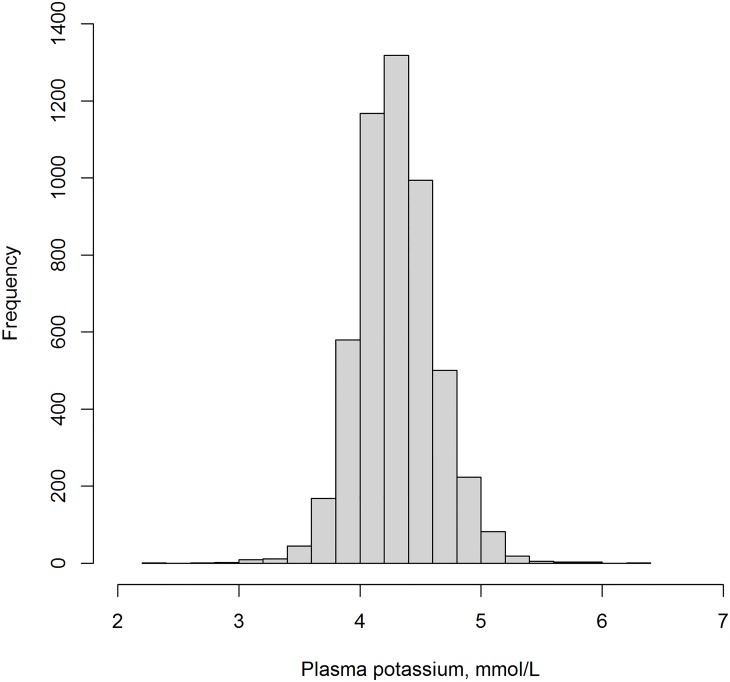
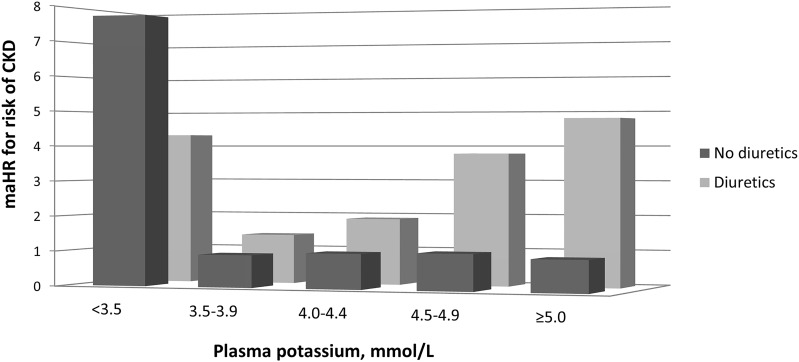
Mean baseline plasma potassium was 4.4±0.3 mmol/L. The prevalences of hypokalemia and hyperkalemia were 0.5% and 3.8%, respectively; 3.0% of the subjects used diuretics. During a median follow-up of 10.3 years (interquartile range: 6.3-11.4 years), 753 subjects developed CKD. The potassium-CKD association was modified by diuretic use (Pinteraction = 0.02). Both hypokalemia without (HR, 7.74, 95% CI, 3.43-17.48) or with diuretic use (HR, 4.32, 95% CI, 1.77-10.51) were associated with an increased CKD risk as compared to plasma potassium 4.0-4.4 mmol/L without diuretic use. Plasma potassium concentrations ≥3.5 mmol/L were associated with an increased CKD risk among subjects using diuretics (Ptrend = 0.01) but not among subjects not using diuretics (Ptrend = 0.74).
In this population-based cohort, hypokalemia was associated with an increased CKD risk, regardless of diuretic use. In the absence of hypokalemia, plasma potassium was not associated with an increased CKD risk, except among subjects using diuretics.
低钾血症和高钾血症均与慢性肾脏病(CKD)患者的疾病进展相关。目前尚不清楚在普通人群中是否存在类似关联。我们的目的是在一个基于人群的队列中研究血钾与CKD发生风险的关联以及利尿剂在此关联中的作用。
我们在预防肾脏和血管终末期疾病(PREVEND)研究的基线时对5130名无CKD的受试者进行了研究,这是一项针对28至75岁荷兰男性和女性的前瞻性、基于人群的队列研究。低钾血症定义为血钾<3.5 mmol/L,高钾血症定义为血钾≥5.0 mmol/L。CKD风险定义为新发估算肾小球滤过率(eGFR)<60 ml/min/1.73m²和/或蛋白尿>30 mg/24小时。
平均基线血钾为4.4±0.3 mmol/L。低钾血症和高钾血症的患病率分别为0.5%和3.8%;3.0%的受试者使用利尿剂。在中位随访10.3年(四分位间距:6.3 - 11.4年)期间,753名受试者发生了CKD。血钾与CKD的关联因利尿剂使用情况而改变(P交互作用 = 0.02)。与未使用利尿剂且血钾为4.0 - 4.4 mmol/L相比,未使用利尿剂的低钾血症(风险比[HR],7.74,95%置信区间[CI],3.43 - 17.48)或使用利尿剂的低钾血症(HR,4.32,95% CI,1.77 - 10.51)均与CKD风险增加相关。血钾浓度≥3.5 mmol/L在使用利尿剂的受试者中与CKD风险增加相关(趋势P = 0.01),但在未使用利尿剂的受试者中无此关联(趋势P = 0.74)。
在这个基于人群的队列中,无论是否使用利尿剂,低钾血症均与CKD风险增加相关。在无低钾血症的情况下,除使用利尿剂的受试者外血钾与CKD风险增加无关。