Center for Personalized Cancer Therapy and Division of Hematology and Oncology, Department of Medicine, University of California, San Diego Moores Cancer Center, La Jolla, California.
Department of Pathology, University of California San Diego Moores Cancer Center, La Jolla, California.
Clin Cancer Res. 2017 Aug 1;23(15):4242-4250. doi: 10.1158/1078-0432.CCR-16-3133. Epub 2017 Mar 28.
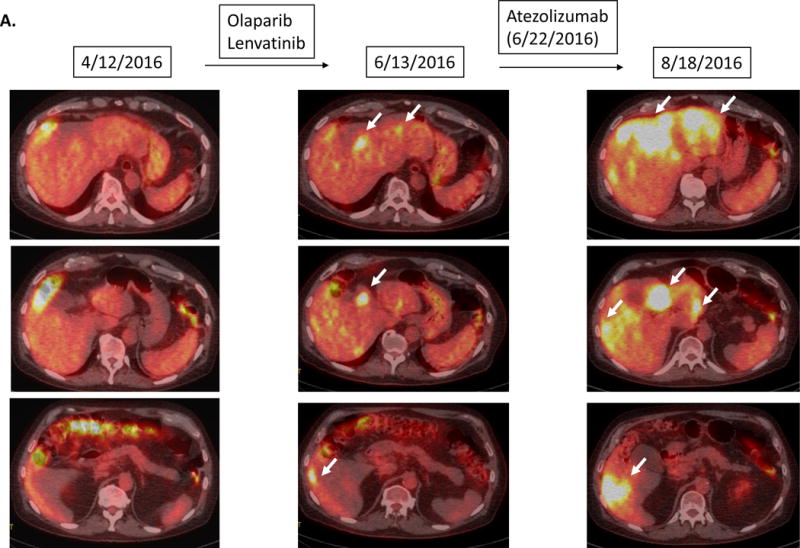
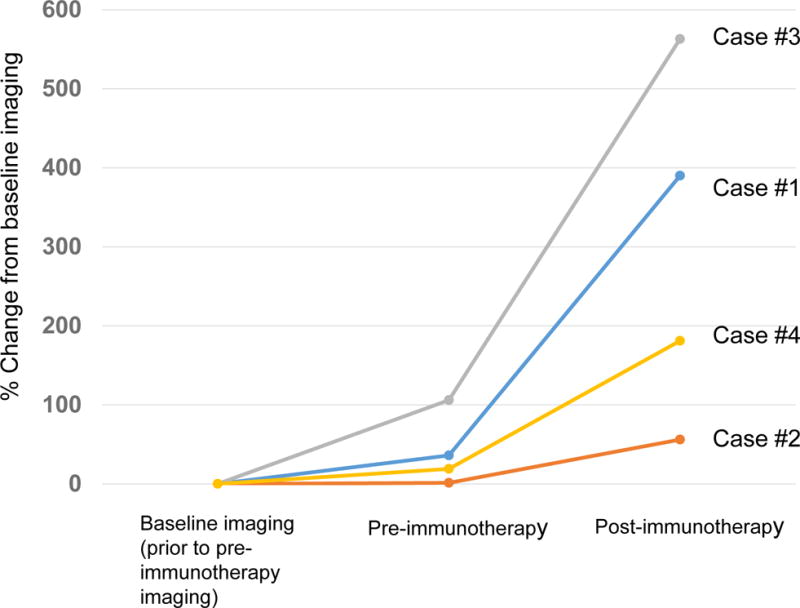
Checkpoint inhibitors demonstrate salutary anticancer effects, including long-term remissions. PD-L1 expression/amplification, high mutational burden, and mismatch repair deficiency correlate with response. We have, however, observed a subset of patients who appear to be "hyperprogressors," with a greatly accelerated rate of tumor growth and clinical deterioration compared with pretherapy, which was also recently reported by Institut Gustave Roussy. The current study investigated potential genomic markers associated with "hyperprogression" after immunotherapy. Consecutive stage IV cancer patients who received immunotherapies (CTLA-4, PD-1/PD-L1 inhibitors or other [investigational] agents) and had their tumor evaluated by next-generation sequencing were analyzed ( = 155). We defined hyperprogression as time-to-treatment failure (TTF) <2 months, >50% increase in tumor burden compared with preimmunotherapy imaging, and >2-fold increase in progression pace. Amongst 155 patients, TTF <2 months was seen in all six individuals with amplification. After anti-PD1/PDL1 monotherapy, four of these patients showed remarkable increases in existing tumor size (55% to 258%), new large masses, and significantly accelerated progression pace (2.3-, 7.1-, 7.2- and 42.3-fold compared with the 2 months before immunotherapy). In multivariate analysis, and alterations correlated with TTF <2 months. Two of 10 patients with alterations were also hyperprogressors (53.6% and 125% increase in tumor size; 35.7- and 41.7-fold increase). Some patients with family amplification or aberrations had poor clinical outcome and significantly increased rate of tumor growth after single-agent checkpoint (PD-1/PD-L1) inhibitors. Genomic profiles may help to identify patients at risk for hyperprogression on immunotherapy. Further investigation is urgently needed. .
检查点抑制剂显示出有益的抗癌作用,包括长期缓解。PD-L1 表达/扩增、高突变负担和错配修复缺陷与反应相关。然而,我们观察到一部分患者似乎是“超进展者”,与治疗前相比,肿瘤生长和临床恶化的速度大大加快,这也最近被 Gustave Roussy 研究所报道。本研究调查了免疫治疗后“超进展”相关的潜在基因组标志物。连续接受免疫治疗(CTLA-4、PD-1/PD-L1 抑制剂或其他[研究性]药物)并通过下一代测序评估肿瘤的 IV 期癌症患者进行了分析(=155)。我们将超进展定义为治疗失败时间(TTF)<2 个月,与免疫治疗前成像相比肿瘤负担增加>50%,进展速度增加>2 倍。在 155 例患者中,所有 6 例 扩增患者的 TTF<2 个月。在抗 PD1/PDL1 单药治疗后,其中 4 例患者现有肿瘤大小显著增加(55%至 258%),出现新的大肿块,且进展速度明显加快(与免疫治疗前 2 个月相比,分别为 2.3、7.1、7.2 和 42.3 倍)。多变量分析显示, 和 改变与 TTF<2 个月相关。10 例 改变患者中有 2 例也是超进展者(肿瘤大小增加 53.6%和 125%;分别增加 35.7 和 41.7 倍)。一些携带 家族扩增或 异常的患者在接受单药检查点(PD-1/PD-L1)抑制剂治疗后临床结局较差,肿瘤生长速度明显加快。基因组谱可能有助于识别免疫治疗中发生超进展的高危患者。迫切需要进一步研究。