Dennison Thomas J, Smith Julian C, Badhan Raj K, Mohammed Afzal R
Aston School of Pharmacy, Aston University, Birmingham.
Viridian Pharma Ltd, Newport, UK.
Drug Des Devel Ther. 2017 Mar 16;11:811-826. doi: 10.2147/DDDT.S126035. eCollection 2017.
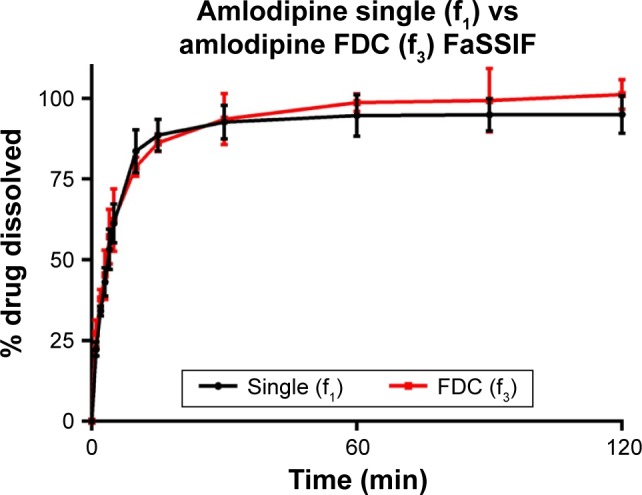
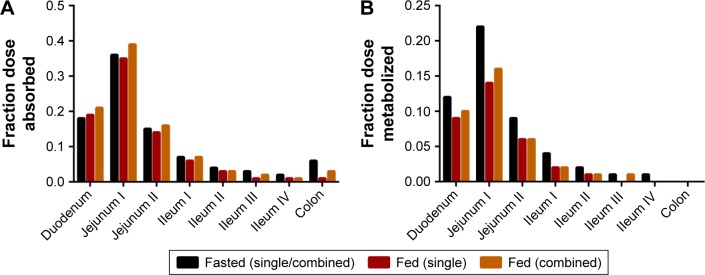
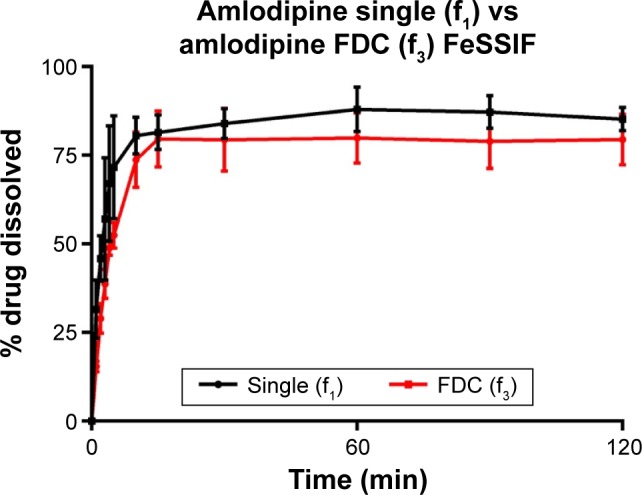
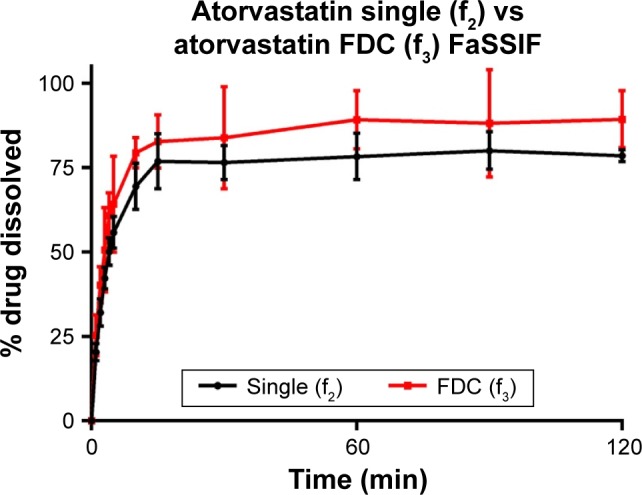
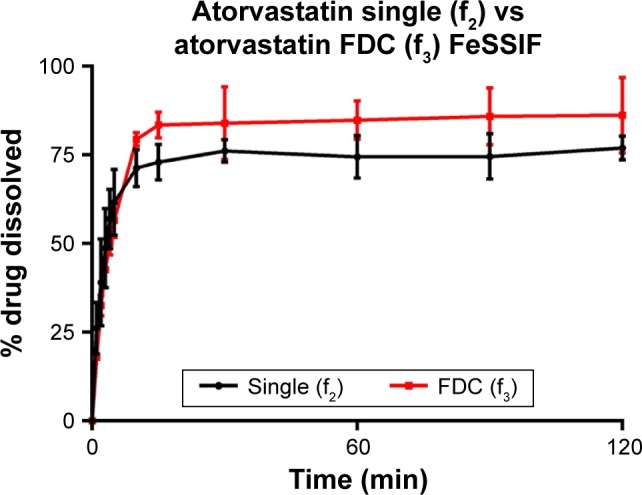
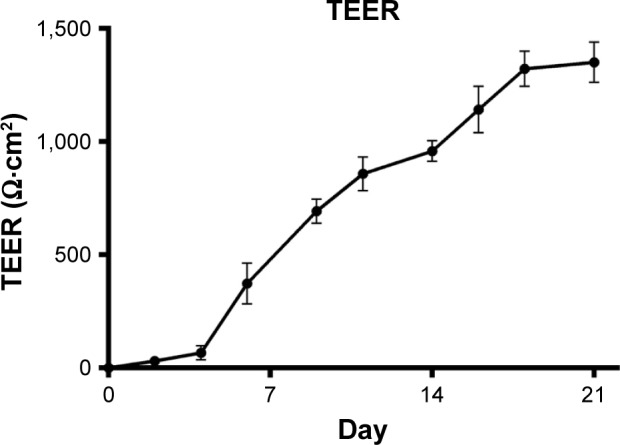
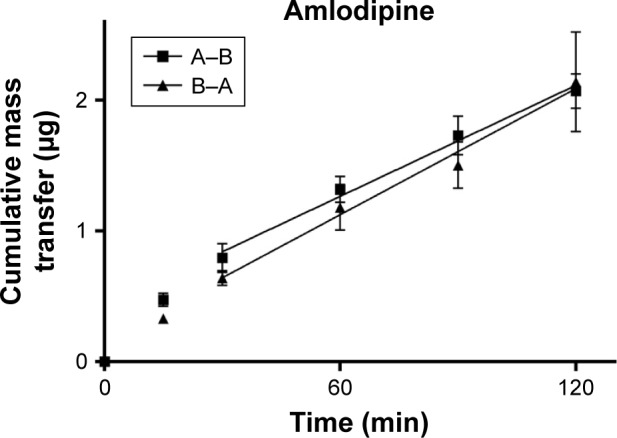
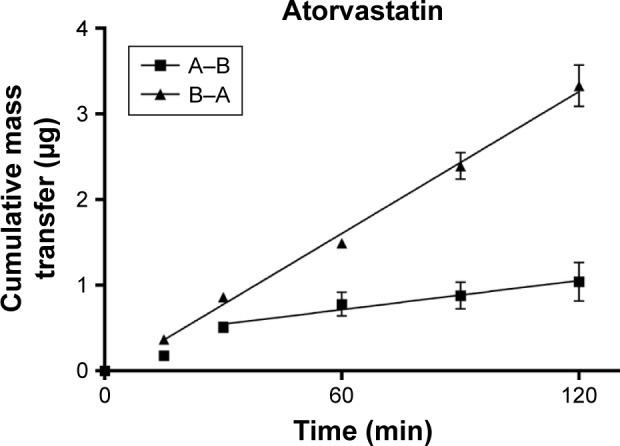
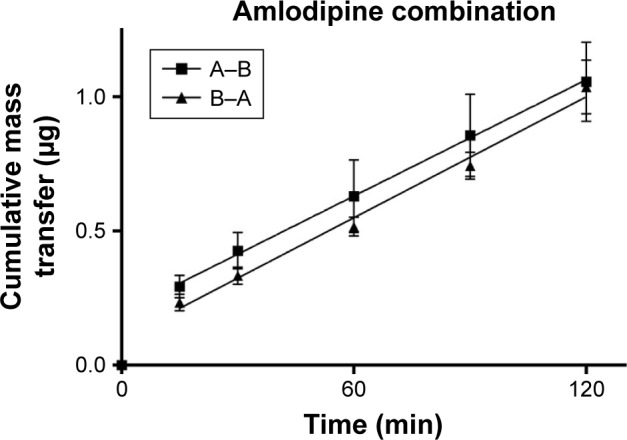
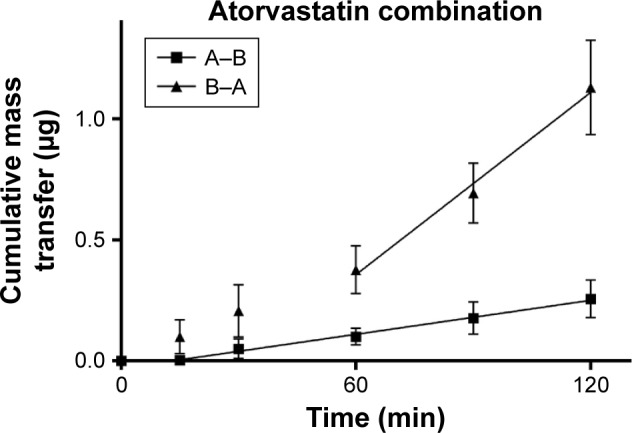
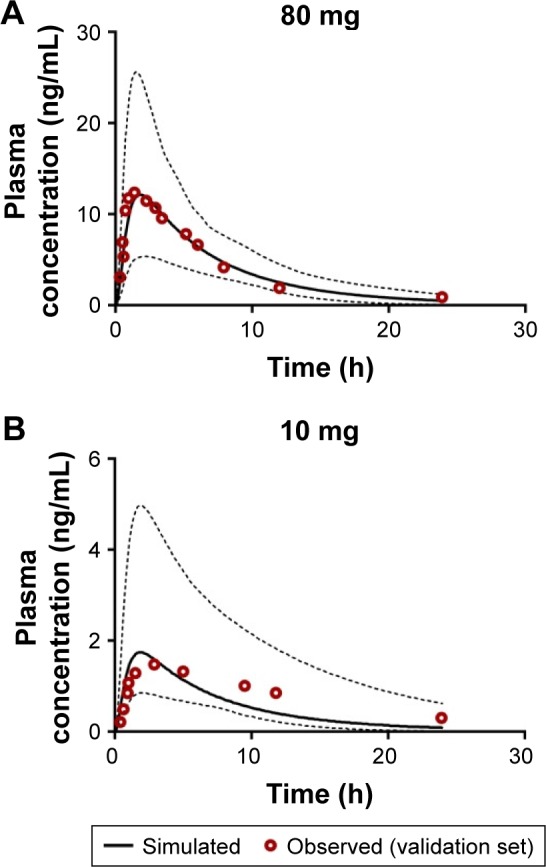
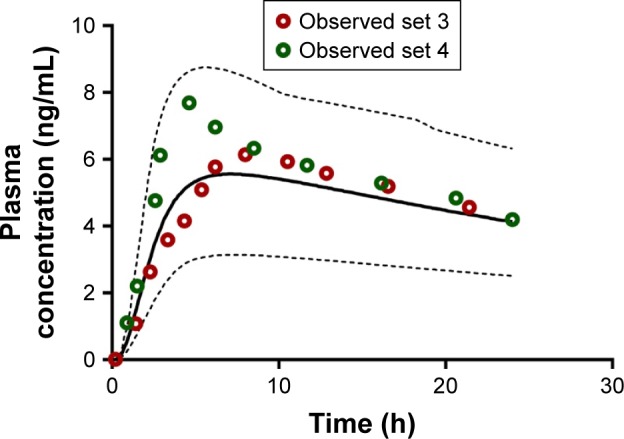
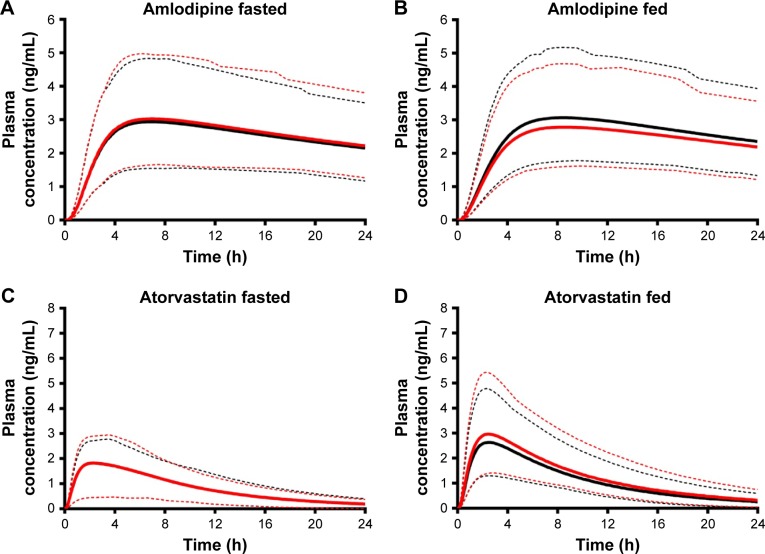
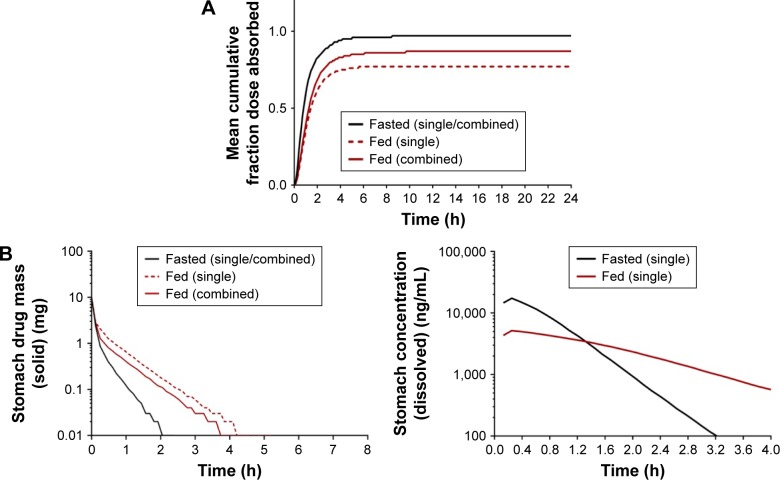
Cardiovascular disease (CVD) is the leading cause of death among men and women worldwide. In CVD, hypertension and dyslipidemia commonly coexist and are managed through coadministration of amlodipine and atorvastatin, respectively. The case for fixed-dose combination (FDC) oral dosage forms and orally disintegrating tablet (ODT) technology to enhance outcomes and compliance is strong. This work follows the development and characterization of single and FDC ODTs containing amlodipine and atorvastatin, followed by bioequivalence comparison between these single and FDC formulations, using in vitro dissolution and Caco-2 apparent permeability (P) and in silico physiologically based pharmacokinetic modeling approaches. ODTs containing amlodipine (5 mg) and atorvastatin (10 mg) either alone or in combination rapidly disintegrated (<30 s) while displaying a radial crushing strength in excess of 100 N and friability ≤1%. In vitro dissolution test was performed in fasted and fed-state simulated intestinal fluid (FeSSIF) and analyzed using high-performance liquid chromatography. Dissolution profiles for single and FDC ODTs were compared using US FDA recommended difference (f) and similarity (f) factor testing for bioequivalence. In all cases, there was no difference in active pharmaceutical ingredient dissolution between single or FDC ODTs, with the exception of amlodipine in FeSSIF. Pharmacokinetic clinical trial simulations were conducted using Simcyp (Version 14), incorporating P and dissolution data. Simulated clinical trials in healthy volunteers showed no difference in bioavailability based on pharmacokinetic parameters between single and combination doses with either active pharmaceutical ingredient. An increase in C and AUC for atorvastatin in fed subjects was attributed to extended transit along the gut lumen and reduced atorvastatin metabolism due to lower CYP3A4 expression at more distal small intestine absorption sites. The results demonstrated bioequivalence of an FDC ODT for amlodipine and atorvastatin, while highlighting several limitations of f and f bioequivalence testing and strengths of mechanistic pharmacokinetic modeling for oral drug absorption.
心血管疾病(CVD)是全球男性和女性的主要死因。在心血管疾病中,高血压和血脂异常通常同时存在,分别通过联合使用氨氯地平和阿托伐他汀进行治疗。固定剂量复方(FDC)口服剂型和口腔崩解片(ODT)技术在改善治疗效果和依从性方面具有显著优势。本研究开展了含氨氯地平和阿托伐他汀的单药及FDC ODT的研发与特性研究,随后采用体外溶出度、Caco-2表观渗透率(P)以及基于生理药代动力学的计算机模拟方法,对这些单药和FDC制剂进行生物等效性比较。含氨氯地平(5 mg)和阿托伐他汀(10 mg)的单药或复方ODT在快速崩解(<30秒)的同时,径向抗压强度超过100 N,脆碎度≤1%。在空腹和进食状态的模拟肠液(FeSSIF)中进行体外溶出试验,并采用高效液相色谱法进行分析。使用美国食品药品监督管理局(US FDA)推荐的差异(f)和相似性(f)因子测试法,比较单药和FDC ODT的溶出曲线以评估生物等效性。在所有情况下,单药或FDC ODT之间的活性药物成分溶出度均无差异,但在FeSSIF中的氨氯地平除外。使用Simcyp(版本14)进行药代动力学临床试验模拟,纳入P和溶出数据。在健康志愿者中进行的模拟临床试验表明,单药剂量和联合剂量的活性药物成分在药代动力学参数方面的生物利用度无差异。进食受试者中阿托伐他汀的Cmax和AUC增加归因于其在肠腔内转运时间延长以及由于小肠远端吸收部位CYP3A4表达降低导致阿托伐他汀代谢减少。结果证明了氨氯地平和阿托伐他汀FDC ODT的生物等效性,同时凸显了f和f生物等效性测试的若干局限性以及口服药物吸收的机械药代动力学建模的优势。